Beckman Kenneth A, Luchs Jodi, Milner Mark S
Comprehensive EyeCare of Central Ohio, Westerville, OH, USA; The Ohio State University, Columbus, OH, USA.
Hofstra University School of Medicine, Hempstead, NY, USA; South Shore Eye Care, Wantagh, NY, USA.
Clin Ophthalmol. 2015 Dec 24;10:43-53. doi: 10.2147/OPTH.S80043. eCollection 2016.
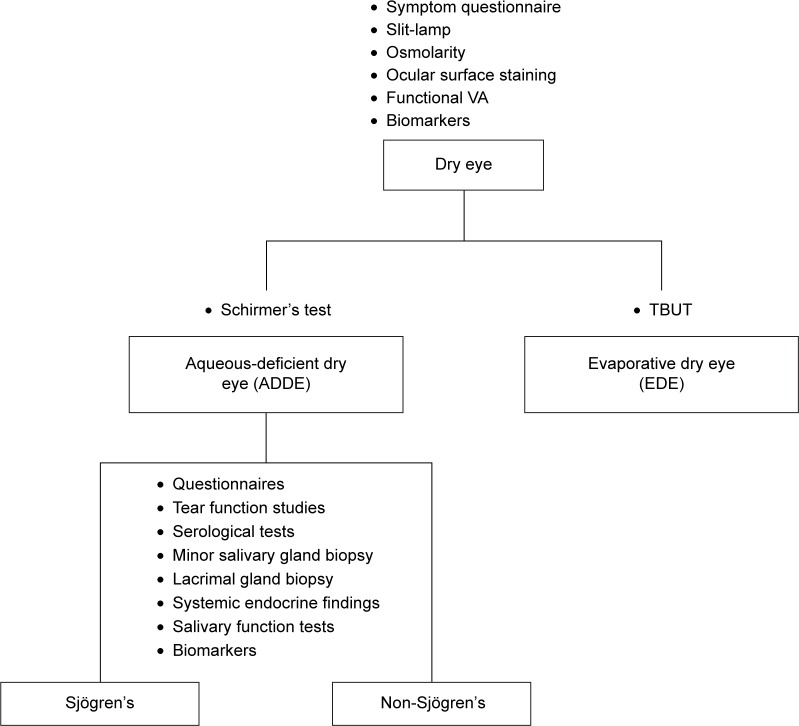
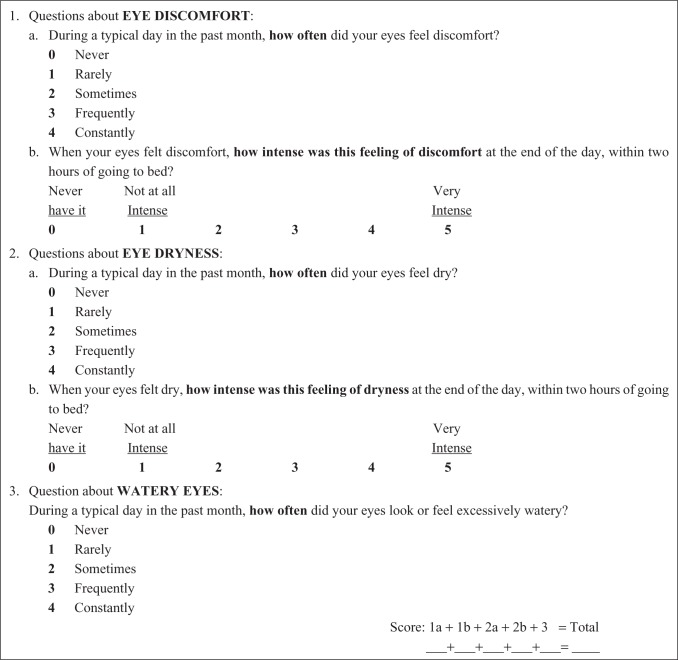
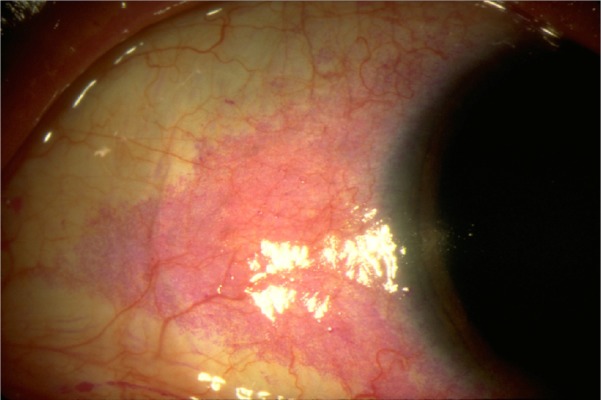
Sjögren's syndrome (SS) is a chronic and progressive systemic autoimmune disease that often presents initially with symptoms of dry eye and dry mouth. Symptoms are often nonspecific and develop gradually, making diagnosis difficult. Patients with dry eye complaints warrant a step-wise evaluation for possible SS. Initial evaluation requires establishment of a dry eye diagnosis using a combination of patient questionnaires and objective ocular tests, including inflammatory biomarker testing. Additional work-up using the Schirmer test and tear film break-up time can differentiate between aqueous-deficient dry eye (ADDE) and evaporative dry eye. The presence of ADDE should trigger further work-up to differentiate between SS-ADDE and non-SS-ADDE. There are numerous non-ocular manifestations of SS, and monitoring for SS-related comorbid findings can aid in diagnosis, ideally in collaboration with a rheumatologist. The clinical work-up of SS can involve a variety of tests, including tear function tests, serological tests for autoantibody biomarkers, minor salivary gland and lacrimal gland biopsies. Examination of classic SS biomarkers (SS-A/Ro, SS-B/La, antinuclear antibody, and rheumatoid factor) is a convenient and non-invasive way of evaluating patients for the presence of SS, even years prior to confirmed diagnosis, although not all SS patients will test positive, particularly those with early disease. Recently, newer biomarkers have been identified, including autoantibodies to salivary gland protein-1, parotid secretory protein, and carbonic anhydrase VI, and may allow for earlier diagnosis of SS. A diagnostic test kit is commercially available (Sjö(®)), incorporating these new biomarkers along with the classic autoantibodies. This advanced test has been shown to identify SS patients who previously tested negative against traditional biomarkers only. All patients with clinically significant ADDE should be considered for serological assessment for SS, given the availability of new serological diagnostic tests and the potentially serious consequences of missing the diagnosis.
干燥综合征(SS)是一种慢性进行性全身性自身免疫性疾病,通常最初表现为干眼和口干症状。症状往往不具特异性且逐渐发展,导致诊断困难。有干眼主诉的患者需要进行逐步评估以排查可能的干燥综合征。初始评估需要结合患者问卷和客观眼部检查(包括炎症生物标志物检测)来确立干眼诊断。使用泪液分泌试验和泪膜破裂时间进行的进一步检查可以区分水液缺乏性干眼(ADDE)和蒸发过强型干眼。ADDE的存在应引发进一步检查,以区分干燥综合征相关性ADDE和非干燥综合征相关性ADDE。干燥综合征有许多非眼部表现,监测与干燥综合征相关的合并症有助于诊断,理想情况下应与风湿病学家合作进行。干燥综合征的临床检查可包括多种检测,如泪液功能测试、自身抗体生物标志物的血清学检测、小唾液腺和泪腺活检。检测典型的干燥综合征生物标志物(SS-A/Ro、SS-B/La、抗核抗体和类风湿因子)是评估患者是否患有干燥综合征的一种便捷且非侵入性的方法,即使在确诊前数年也是如此,尽管并非所有干燥综合征患者都会检测呈阳性,尤其是那些早期疾病患者。最近,已鉴定出更新的生物标志物,包括针对唾液腺蛋白-1、腮腺分泌蛋白和碳酸酐酶VI的自身抗体,可能有助于干燥综合征的早期诊断。一种诊断试剂盒已上市(Sjö(®)),它将这些新生物标志物与经典自身抗体结合在一起。这种先进的检测已被证明能够识别那些之前仅对传统生物标志物检测呈阴性的干燥综合征患者。鉴于新的血清学诊断检测方法的可用性以及漏诊可能产生的潜在严重后果,所有具有临床意义的ADDE患者都应考虑进行干燥综合征的血清学评估。