Dental Informatics, Department of Cariology, Operative Dentistry & Dental Public Health, Indiana University School of Dentistry, Indianapolis, Indiana, United States of America.
Center for Biomedical Informatics, Regenstrief Institute Inc., Indianapolis, Indiana, United States of America.
PLoS One. 2023 Jul 31;18(7):e0289335. doi: 10.1371/journal.pone.0289335. eCollection 2023.
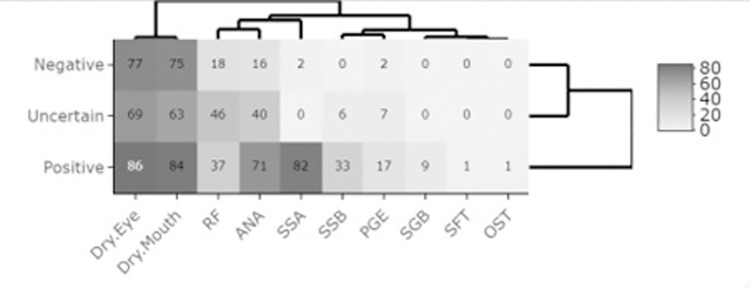
Established classifications exist to confirm Sjögren's Disease (SD) (previously referred as Sjögren's Syndrome) and recruit patients for research. However, no established classification exists for diagnosis in clinical settings causing delayed diagnosis. SD patients experience a huge dental disease burden impairing their quality of life. This study established criteria to characterize Indiana University School of Dentistry (IUSD) patients' SD based on symptoms and signs in the electronic health record (EHR) data available through the state-wide Indiana health information exchange (IHIE). Association between SD diagnosis, and comorbidities including other autoimmune conditions, and documentation of SD diagnosis in electronic dental record (EDR) were also determined. The IUSD patients' EDR were linked with their EHR data in the IHIE and queried for SD diagnostic ICD9/10 codes. The resulting cohorts' EHR clinical findings were characterized and classified using diagnostic criteria based on clinical experts' recommendations. Descriptive statistics were performed, and Chi-square tests determined the association between the different SD presentations and comorbidities including other autoimmune conditions. Eighty-three percent of IUSD patients had an EHR of which 377 patients had a SD diagnosis. They were characterized as positive (24%), uncertain (20%) and negative (56%) based on EHR clinical findings. Dry eyes and mouth were reported for 51% and positive Anti-Ro/SSA antibodies and anti-nuclear antibody (ANA) for 17% of this study cohort. One comorbidity was present in 98% and other autoimmune condition/s were present in 53% respectively. Significant differences were observed between the three SD clinical characteristics/classifications and certain medical and autoimmune conditions (p<0.05). Sixty-nine percent of patients' EDR did not mention SD, highlighting the huge gap in reporting SD during dental care. This study of SD patients diagnosed in community practices characterized three different SD clinical presentations, which can be used to generate SD study cohorts for longitudinal studies using EHR data. The results emphasize the heterogenous SD clinical presentations and the need for further research to diagnose SD early in community practice settings where most people seek care.
现有的分类方法可用于确认干燥综合征(SD)(以前称为干燥综合征)并招募研究患者。然而,在临床环境中,尚无用于诊断的既定分类方法,这导致了诊断的延迟。SD 患者患有严重的口腔疾病,这降低了他们的生活质量。本研究基于通过州范围内的印第安纳州健康信息交换(IHIE)获得的电子健康记录(EHR)数据中可用的症状和体征,建立了印第安纳大学牙科学院(IUSD)患者 SD 的特征分类标准。还确定了 SD 诊断、与其他自身免疫性疾病的合并症以及电子牙科记录(EDR)中 SD 诊断记录之间的关联。IUSD 患者的 EDR 与 IHIE 中的 EHR 数据相关联,并查询 SD 诊断 ICD9/10 代码。使用基于临床专家建议的诊断标准对队列的 EHR 临床发现进行了特征描述和分类。进行了描述性统计分析,卡方检验确定了不同 SD 表现与合并症(包括其他自身免疫性疾病)之间的关联。83%的 IUSD 患者有 EHR,其中 377 名患者有 SD 诊断。根据 EHR 临床发现,他们被归类为阳性(24%)、不确定(20%)和阴性(56%)。本研究队列中有 51%的患者报告有干眼症和口干,17%的患者有抗 Ro/SSA 抗体和抗核抗体(ANA)阳性。98%的患者存在一种合并症,53%的患者存在一种或多种其他自身免疫性疾病。在三种 SD 临床特征/分类和某些医学和自身免疫性疾病之间观察到显著差异(p<0.05)。69%的患者的 EDR 未提及 SD,这突显了在牙科护理中报告 SD 的巨大差距。本研究对社区实践中诊断的 SD 患者进行了研究,对三种不同的 SD 临床表现进行了特征描述,这可用于使用 EHR 数据生成 SD 研究队列进行纵向研究。研究结果强调了 SD 临床表现的异质性,需要进一步研究,以便在大多数人寻求医疗服务的社区实践环境中尽早诊断 SD。