Department of Health Sciences, University of Leicester, Leicester, UK.
Department of Health Services Research, Management and Policy, University of Florida, Gainesville, Florida, USA Department of Community Health and Family Medicine, University of Florida, Gainesville, Florida, USA.
BMJ Open. 2016 Feb 11;6(2):e009981. doi: 10.1136/bmjopen-2015-009981.
Health systems with strong primary care tend to have better population outcomes, but in many countries demand for care is growing. We sought to identify mechanisms of primary care that influence premature mortality.
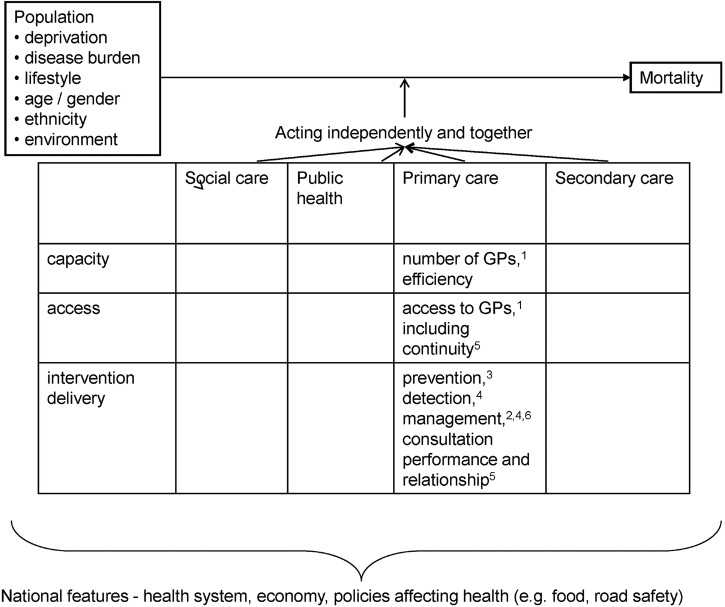
We developed a conceptual model of the mechanisms by which primary care influences premature mortality, and undertook a cross-sectional study in which population and primary care variables reflecting the model were used to explain variations in mortality of those aged under 75 years. The premature standardised mortality ratios (SMRs) for each practice, available from the Department of Health, had been calculated from numbers of deaths in the 5 years from 2006 to 2010. A regression model was undertaken with explanatory variables for the year 2009/2010, and repeated to check stability using data for 2008/2009 and 2010/2011.
All general practices in England were eligible for inclusion and, of the total of 8290, complete data were available for 7858.
Population variables, particularly deprivation, were the most powerful predictors of premature mortality, but the mechanisms of primary care depicted in our model also affected mortality. The number of GPs/1000 population and detection of hypertension were negatively associated with mortality. In less deprived practices, continuity of care was also negatively associated with mortality.
Greater supply of primary care is associated with lower premature mortality even in a health system that has strong primary care (England). Health systems need to sustain the capacity of primary care to deliver effective care, and should assist primary care providers in identifying and meeting the needs of socioeconomically deprived groups.
拥有强大基层医疗服务的卫生系统往往能产生更好的人群健康结果,但在许多国家,医疗服务需求正在不断增长。我们试图确定影响过早死亡的基层医疗服务的作用机制。
我们开发了一个基层医疗服务影响过早死亡的作用机制概念模型,并进行了一项横断面研究,其中使用反映该模型的人群和基层医疗服务变量来解释 75 岁以下人群的死亡率差异。卫生署提供的每个实践的过早标准化死亡率比(SMR)是根据 2006 年至 2010 年 5 年内的死亡人数计算得出的。采用回归模型对 2009/2010 年的解释变量进行了分析,并使用 2008/2009 年和 2010/2011 年的数据进行了重复,以检查稳定性。
英格兰所有的普通实践都有资格入选,在总共 8290 个实践中,有 7858 个实践提供了完整的数据。
人群变量,特别是贫困程度,是过早死亡的最强预测因素,但我们模型中描述的基层医疗服务作用机制也会影响死亡率。每千人口的全科医生数量和高血压的检出率与死亡率呈负相关。在贫困程度较低的实践中,连续性护理也与死亡率呈负相关。
即使在拥有强大基层医疗服务的卫生系统(英国)中,更多的基层医疗服务供应也与更低的过早死亡率相关。卫生系统需要维持基层医疗服务提供有效医疗服务的能力,并应帮助基层医疗服务提供者识别和满足社会经济贫困群体的需求。