Disertori Marcello, Gulizia Michele M, Casolo Giancarlo, Delise Pietro, Di Lenarda Andrea, Di Tano Giuseppe, Lunati Maurizio, Mestroni Luisa, Salerno-Uriarte Jorge, Tavazzi Luigi
aCardiology Department, S. Chiara Hospital - Healthcare Research and Innovation Program, PAT-FBK, Trento bCardiology Department, Garibaldi-Nesima Hospital, Catania cU.O. of Cardiology, Versilia Hospital, Lido di Camaiore (LU) dDivision of Cardiology, Pederzoli Hospital, Peschiera del Garda (VR) eCardiovascular Center, Azienda Servizi Sanitari N.1 - University of Trieste, Trieste fU.O of Cardiology, Azienda Istituti Ospitalieri, Cremona gCardiology Department, Niguarda Ca' Granda Hospital, Milano, Italy hCardiovascular Institute, University of Colorado Denver AMC, Aurora, Colorado, USA iDepartment of Heart Science, Ospedale di Circolo e Fondazione Macchi, University of Insubria, Varese jGVM, Maria Cecilia Hospital, Care and Research - ES Health Science Foundation, Cotignola (RA), Italy.
J Cardiovasc Med (Hagerstown). 2016 Apr;17(4):245-55. doi: 10.2459/JCM.0000000000000368.
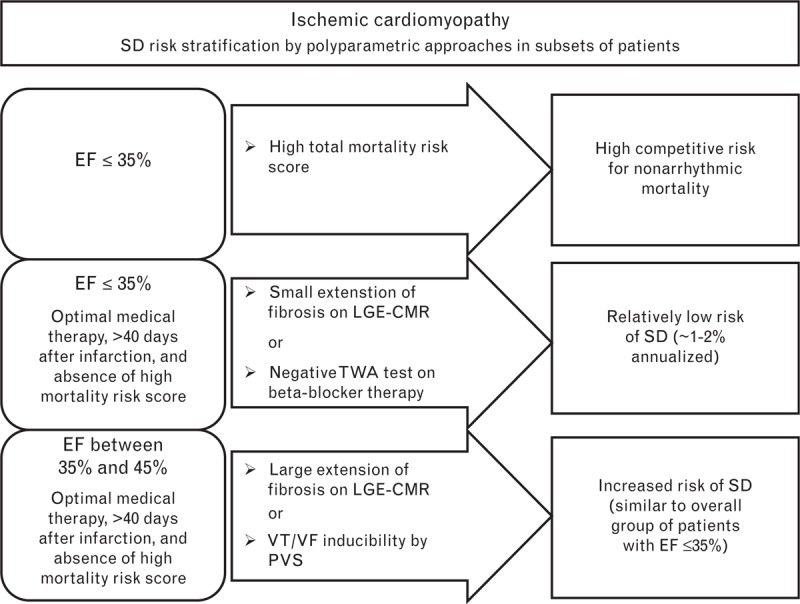
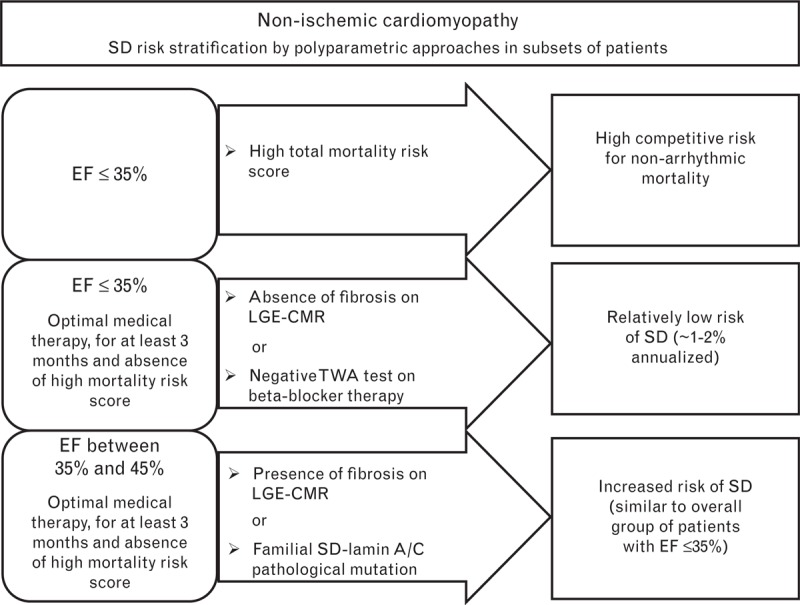
It is generally accepted that the current guidelines for the primary prevention of sudden arrhythmic death, which are based on ejection fraction, do not allow the optimal selection of patients with low left ventricular ejection fraction of ischemic and nonischemic etiology for implantation of a cardioverter-defibrillator. Ejection fraction alone is limited in both sensitivity and specificity. An analysis of the risk of sudden arrhythmic death with a combination of multiple tests (ejection fraction associated with one or more arrhythmic risk markers) could partially compensate for these limitations. We propose a polyparametric approach for defining the risk of sudden arrhythmic death using ejection fraction in combination with other clinical and arrhythmic risk markers (i.e. late gadolinium enhancement cardiac magnetic resonance, T-wave alternans, programmed ventricular stimulation, autonomic tone, and genetic testing) that have been validated in nonrandomized trials. In this article, we examine these approaches to identify three subsets of patients who cannot be comprehensively assessed by the current guidelines: patients with ejection fraction of 35% or less and a relatively low risk of sudden arrhythmic death despite the ejection fraction value; patients with ejection fraction of 35% or less and high competitive risk of death due to evolution of heart failure or noncardiac causes; and patients with ejection fraction between 35 and 45% with relatively high risk of sudden arrhythmic death despite the ejection fraction value.
目前普遍认为,基于射血分数的当前心律失常性猝死一级预防指南,无法对缺血性和非缺血性病因导致左心室射血分数降低的患者进行最佳筛选,以确定是否适合植入心脏复律除颤器。仅射血分数在敏感性和特异性方面都存在局限性。对多种检测方法(射血分数与一种或多种心律失常风险标志物相结合)综合分析心律失常性猝死风险,可部分弥补这些局限性。我们提出一种多参数方法,使用射血分数结合其他临床和心律失常风险标志物(即延迟钆增强心脏磁共振成像、T波电交替、程控心室刺激、自主神经张力和基因检测)来定义心律失常性猝死风险,这些标志物已在非随机试验中得到验证。在本文中,我们研究这些方法,以识别出当前指南无法全面评估的三类患者:射血分数为35%或更低,但尽管射血分数值如此,心律失常性猝死风险相对较低的患者;射血分数为35%或更低,但因心力衰竭进展或非心脏原因导致死亡的竞争风险较高的患者;以及射血分数在35%至45%之间,尽管射血分数值如此,但心律失常性猝死风险相对较高的患者。