Palmqvist Sebastian, Mattsson Niklas, Hansson Oskar
Clinical Memory Research Unit, Department of Clinical Sciences, Malmö, Lund University, Sweden Department of Neurology, Skåne University Hospital, Sweden
Clinical Memory Research Unit, Department of Clinical Sciences, Malmö, Lund University, Sweden Memory Clinic, Skåne University Hospital, Sweden.
Brain. 2016 Apr;139(Pt 4):1226-36. doi: 10.1093/brain/aww015. Epub 2016 Mar 2.
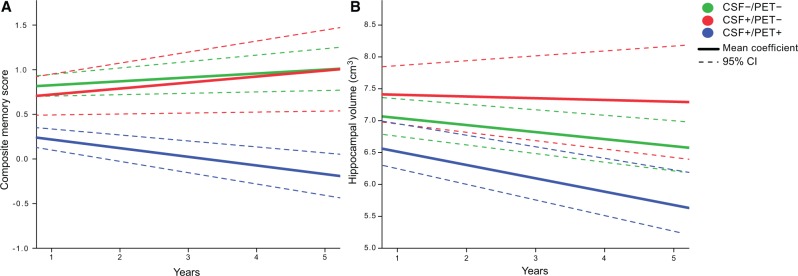
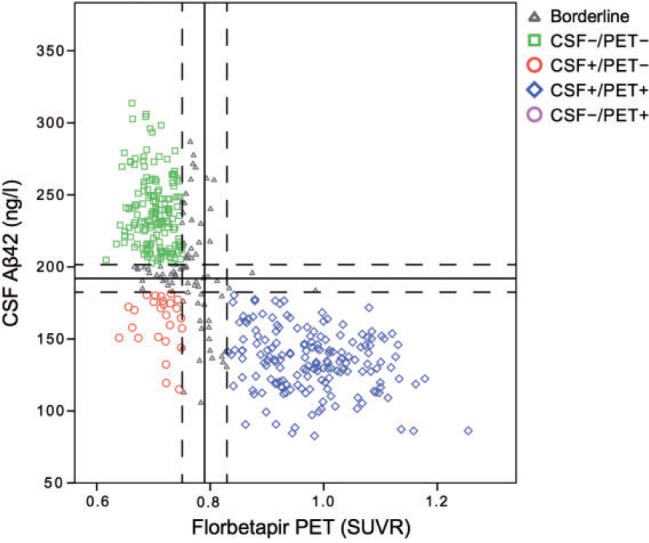
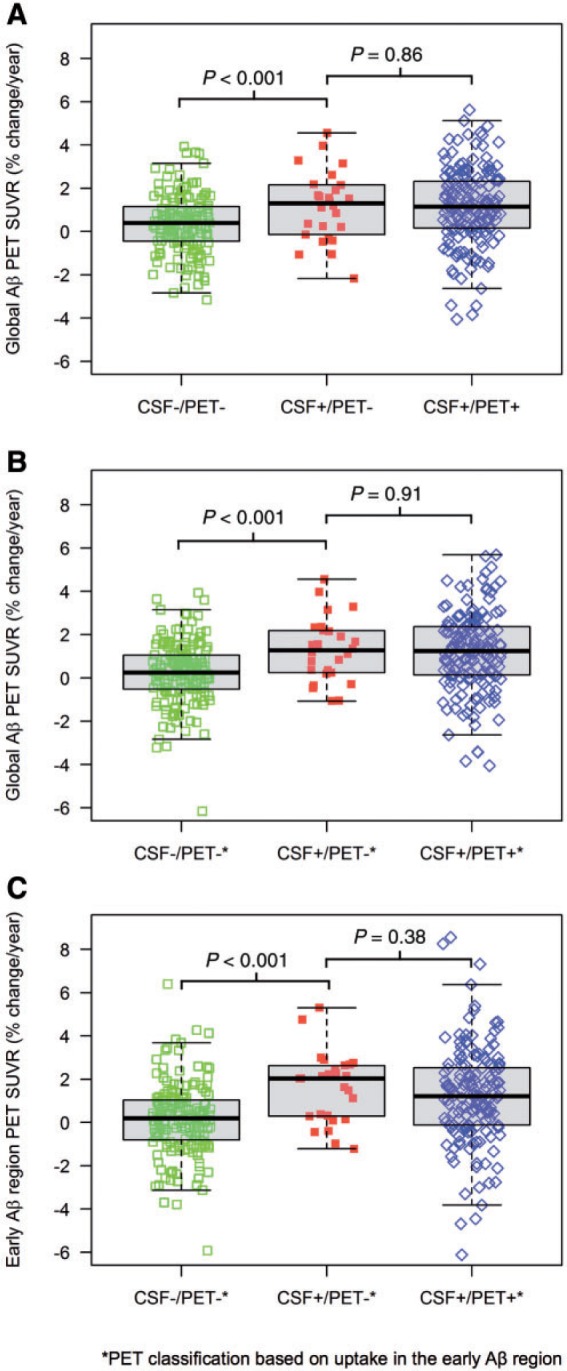
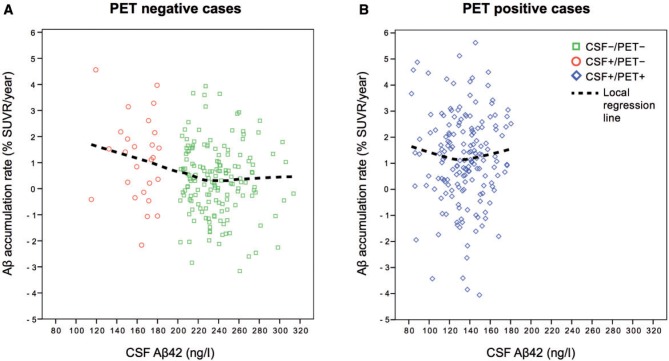
Cerebral accumulation of amyloid-β is thought to be the starting mechanism in Alzheimer's disease. Amyloid-β can be detected by analysis of cerebrospinal fluid amyloid-β42 or amyloid positron emission tomography, but it is unknown if any of the methods can identify an abnormal amyloid accumulation prior to the other. Our aim was to determine whether cerebrospinal fluid amyloid-β42 change before amyloid PET during preclinical stages of Alzheimer's disease. We included 437 non-demented subjects from the prospective, longitudinal Alzheimer's Disease Neuroimaging Initiative (ADNI) study. All underwent (18)F-florbetapir positron emission tomography and cerebrospinal fluid amyloid-β42 analysis at baseline and at least one additional positron emission tomography after a mean follow-up of 2.1 years (range 1.1-4.4 years). Group classifications were based on normal and abnormal cerebrospinal fluid and positron emission tomography results at baseline. We found that cases with isolated abnormal cerebrospinal fluid amyloid-β and normal positron emission tomography at baseline accumulated amyloid with a mean rate of 1.2%/year, which was similar to the rate in cases with both abnormal cerebrospinal fluid and positron emission tomography (1.2%/year, P = 0.86). The mean accumulation rate of those with isolated abnormal cerebrospinal fluid was more than three times that of those with both normal cerebrospinal fluid and positron emission tomography (0.35%/year, P = 0.018). The group differences were similar when analysing yearly change in standardized uptake value ratio of florbetapir instead of percentage change. Those with both abnormal cerebrospinal fluid and positron emission tomography deteriorated more in memory and hippocampal volume compared with the other groups (P < 0.001), indicating that they were closer to Alzheimer's disease dementia. The results were replicated after adjustments of different factors and when using different cut-offs for amyloid-β abnormality including a positron emission tomography classification based on the florbetapir uptake in regions where the initial amyloid-β accumulation occurs in Alzheimer's disease. This is the first study to show that individuals who have abnormal cerebrospinal amyloid-β42 but normal amyloid-β positron emission tomography have an increased cortical amyloid-β accumulation rate similar to those with both abnormal cerebrospinal fluid and positron emission tomography and higher rate than subjects where both modalities are normal. The results indicate that cerebrospinal fluid amyloid-β42 becomes abnormal in the earliest stages of Alzheimer's disease, before amyloid positron emission tomography and before neurodegeneration starts.
淀粉样蛋白β在大脑中的蓄积被认为是阿尔茨海默病的起始机制。可通过分析脑脊液淀粉样蛋白β42或淀粉样蛋白正电子发射断层扫描来检测淀粉样蛋白β,但尚不清楚这些方法中的任何一种是否能先于另一种检测到异常的淀粉样蛋白蓄积。我们的目的是确定在阿尔茨海默病临床前阶段,脑脊液淀粉样蛋白β42是否在淀粉样蛋白PET之前发生变化。我们纳入了前瞻性纵向阿尔茨海默病神经影像学倡议(ADNI)研究中的437名非痴呆受试者。所有人在基线时均接受了(18)F-氟比他哌正电子发射断层扫描和脑脊液淀粉样蛋白β42分析,并在平均随访2.1年(范围1.1 - 4.4年)后至少又接受了一次正电子发射断层扫描。分组分类基于基线时脑脊液和正电子发射断层扫描结果的正常与异常情况。我们发现,基线时脑脊液淀粉样蛋白β单独异常而正电子发射断层扫描正常的病例,淀粉样蛋白蓄积的平均速率为每年1.2%,这与脑脊液和正电子发射断层扫描均异常的病例的速率相似(每年1.2%,P = 0.86)。脑脊液单独异常者的平均蓄积速率是脑脊液和正电子发射断层扫描均正常者的三倍多(每年0.35%,P = 0.018)。在分析氟比他哌标准化摄取值比率的年度变化而非百分比变化时,组间差异相似。与其他组相比,脑脊液和正电子发射断层扫描均异常者在记忆和海马体积方面恶化更明显(P < 0.001),这表明他们更接近阿尔茨海默病痴呆。在对不同因素进行调整后,以及在使用不同的淀粉样蛋白β异常临界值(包括基于阿尔茨海默病中最初淀粉样蛋白β蓄积区域的氟比他哌摄取的正电子发射断层扫描分类)时,结果得到了重复验证。这是第一项表明脑脊液淀粉样蛋白β42异常但淀粉样蛋白β正电子发射断层扫描正常的个体,其皮质淀粉样蛋白β蓄积速率增加,与脑脊液和正电子发射断层扫描均异常者相似且高于两种检查均正常的受试者的研究。结果表明,在阿尔茨海默病的最早阶段,在淀粉样蛋白正电子发射断层扫描之前以及神经退行性变开始之前,脑脊液淀粉样蛋白β42就已变得异常。