Palmeri Mark L, Glass Tyler J, Miller Zachary A, Rosenzweig Stephen J, Buck Andrew, Polascik Thomas J, Gupta Rajan T, Brown Alison F, Madden John, Nightingale Kathryn R
Department of Biomedical Engineering, Duke University, Durham, North Carolina, USA.
Department of Biomedical Engineering, Duke University, Durham, North Carolina, USA.
Ultrasound Med Biol. 2016 Jun;42(6):1251-62. doi: 10.1016/j.ultrasmedbio.2016.01.004. Epub 2016 Mar 3.
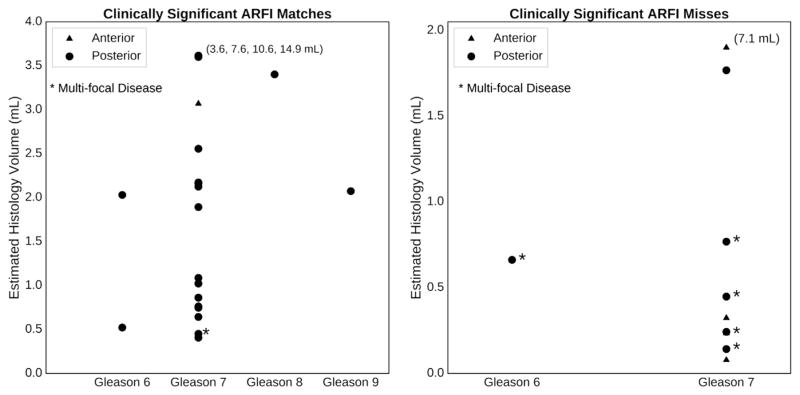
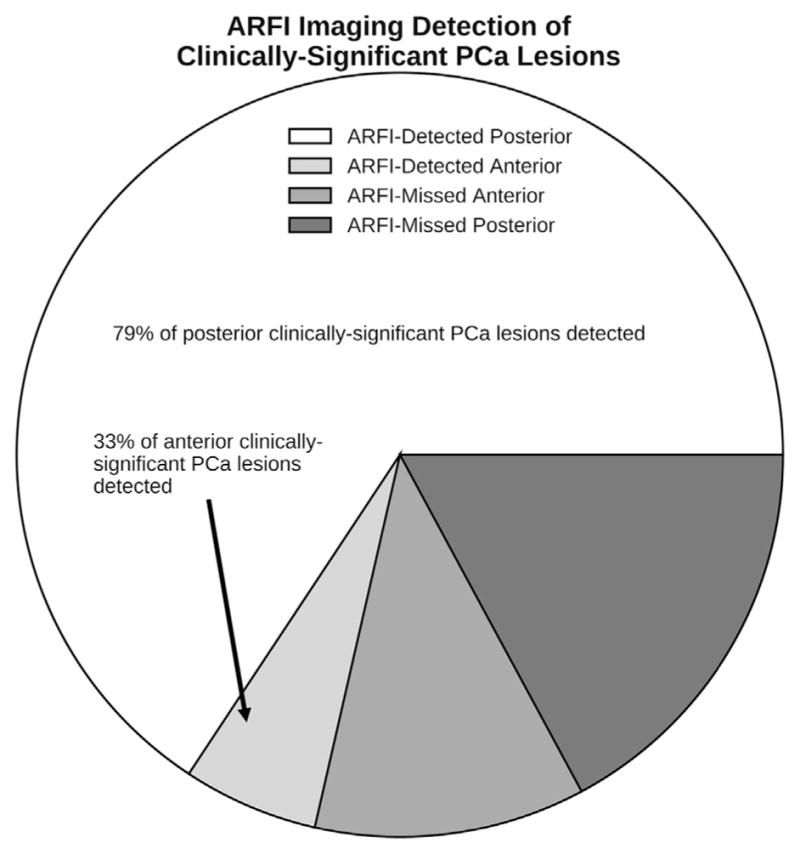
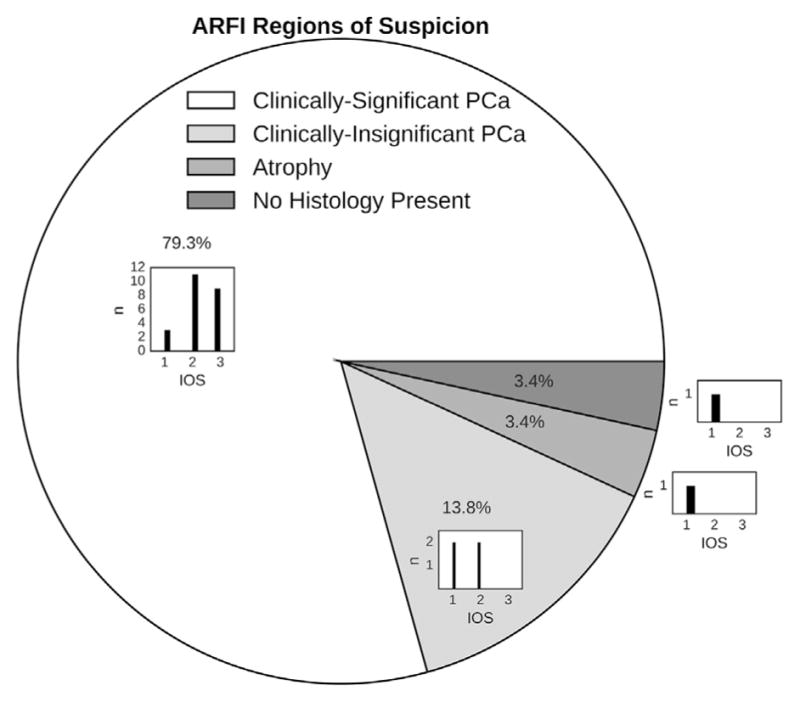
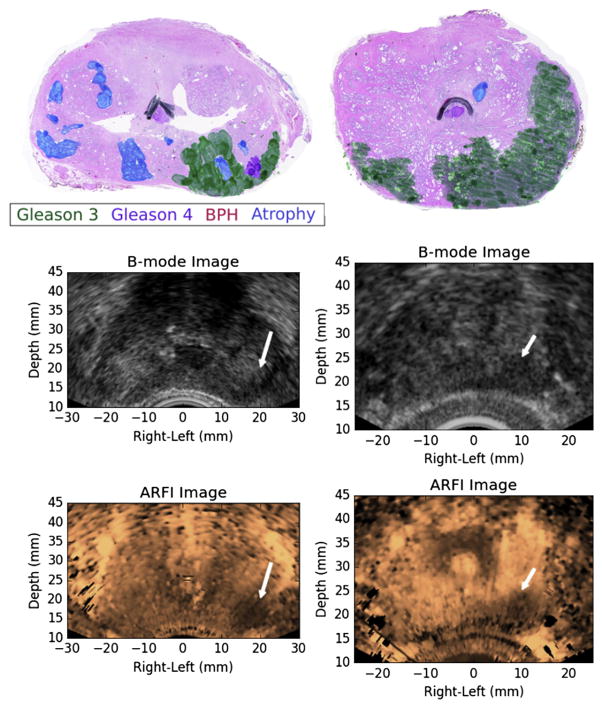
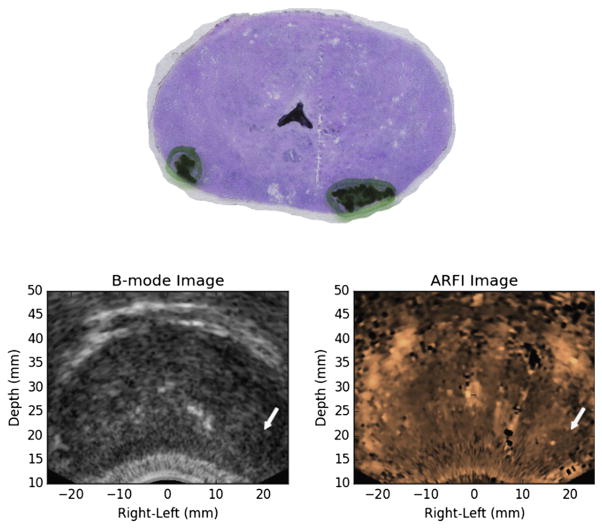
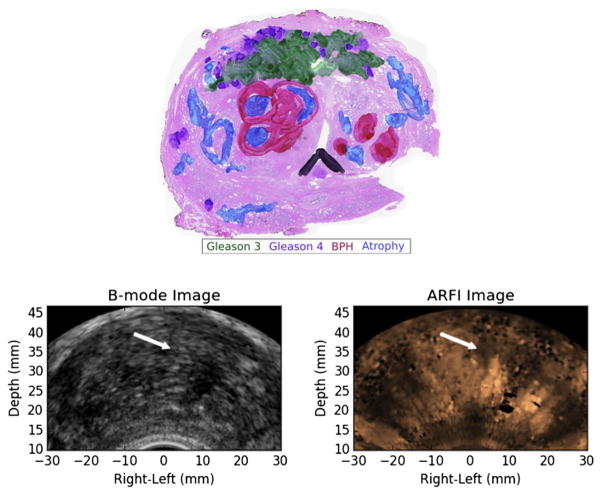
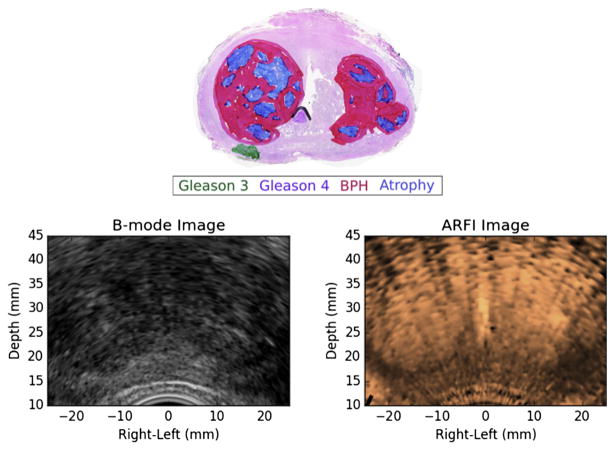
Overly aggressive prostate cancer (PCa) treatment adversely affects patients and places an unnecessary burden on our health care system. The inability to identify and grade clinically significant PCa lesions is a factor contributing to excessively aggressive PCa treatment, such as radical prostatectomy, instead of more focal, prostate-sparing procedures such as cryotherapy and high-dose radiation therapy. We have performed 3-D in vivo B-mode and acoustic radiation force impulse (ARFI) imaging using a mechanically rotated, side-fire endorectal imaging array to identify regions suspicious for PCa in 29 patients being treated with radical prostatectomies for biopsy-confirmed PCa. Whole-mount histopathology analyses were performed to identify regions of clinically significant/insignificant PCa lesions, atrophy and benign prostatic hyperplasia. Regions of suspicion for PCa were reader-identified in ARFI images based on boundary delineation, contrast, texture and location. These regions of suspicion were compared with histopathology identified lesions using a nearest-neighbor regional localization approach. Of all clinically significant lesions identified on histopathology, 71.4% were also identified using ARFI imaging, including 79.3% of posterior and 33.3% of anterior lesions. Among the ARFI-identified lesions, 79.3% corresponded to clinically significant PCa lesions, with these lesions having higher indices of suspicion than clinically insignificant PCa. ARFI imaging had greater sensitivity for posterior versus anterior lesions because of greater displacement signal-to-noise ratio and finer spatial sampling. Atrophy and benign prostatic hyperplasia can cause appreciable prostate anatomy distortion and heterogeneity that confounds ARFI PCa lesion identification; however, in general, ARFI regions of suspicion did not coincide with these benign pathologies.
过度积极的前列腺癌(PCa)治疗会对患者产生不利影响,并给我们的医疗保健系统带来不必要的负担。无法识别和分级具有临床意义的PCa病变是导致过度积极的PCa治疗的一个因素,例如根治性前列腺切除术,而不是采用更局部的、保留前列腺的手术,如冷冻疗法和高剂量放射治疗。我们使用机械旋转的侧射式直肠内成像阵列进行了三维体内B模式和声辐射力脉冲(ARFI)成像,以识别29例经活检确诊为PCa并接受根治性前列腺切除术的患者中可疑的PCa区域。进行了全层组织病理学分析,以识别具有临床意义/无临床意义的PCa病变、萎缩和良性前列腺增生区域。基于边界描绘(边界划分)、对比度、纹理和位置,在ARFI图像中由阅片者识别出可疑的PCa区域。使用最近邻区域定位方法将这些可疑区域与组织病理学确定的病变进行比较。在组织病理学上确定的所有具有临床意义的病变中,71.4%也通过ARFI成像被识别出来,其中包括79.3%的后部病变和33.3%的前部病变。在ARFI识别出的病变中,79.3%对应于具有临床意义的PCa病变,这些病变的可疑指数高于无临床意义的PCa。由于更高的位移信噪比和更精细的空间采样,ARFI成像对后部病变的敏感性高于前部病变。萎缩和良性前列腺增生可导致明显的前列腺解剖结构扭曲和异质性,这会混淆ARFI对PCa病变的识别;然而,总体而言,ARFI可疑区域与这些良性病变并不一致。 (注:括号内为补充完善使译文更通顺的内容)