Arbovirus and Viral Hemorrhagic Fever Unit, Institut Pasteur de Dakar, Dakar, Senegal.
INSERM, U1136, Paris, France; Sorbonne Universités, UPMC Paris 06, Institut Pierre Louis d'Epidémiologie et de Santé Publique, Paris, France.
Lancet Infect Dis. 2015 Mar;15(3):320-6. doi: 10.1016/S1473-3099(14)71075-8. Epub 2015 Jan 23.
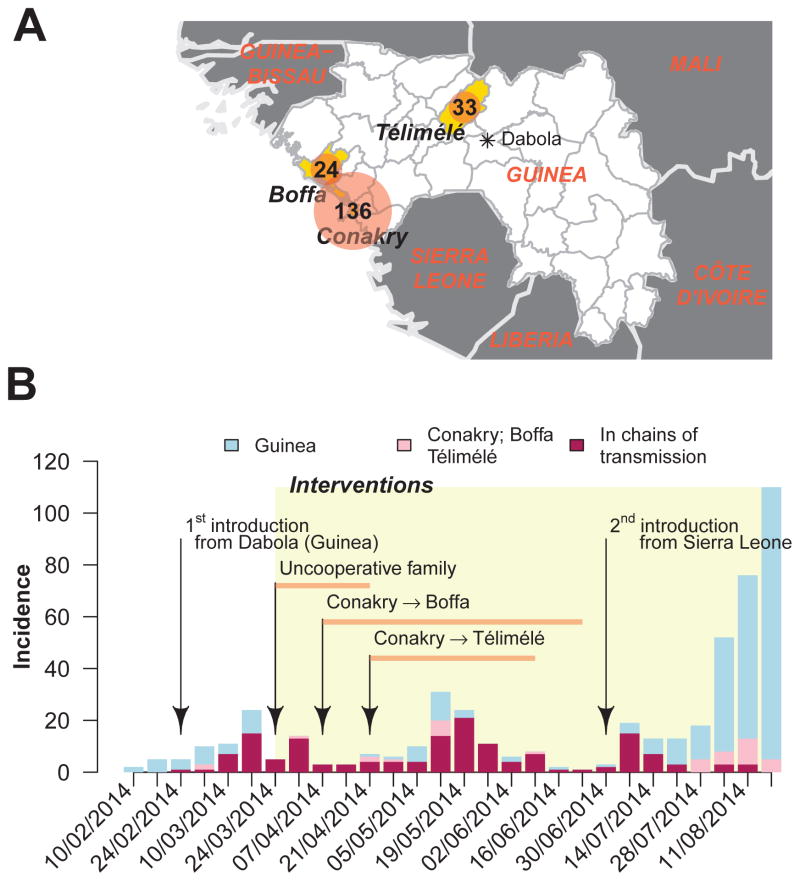
An epidemic of Ebola virus disease of unprecedented size continues in parts of west Africa. For the first time, large urban centres such as Conakry, the capital of Guinea, are affected. We did an observational study of patients with Ebola virus disease in three regions of Guinea, including Conakry, aiming to map the routes of transmission and assess the effect of interventions.
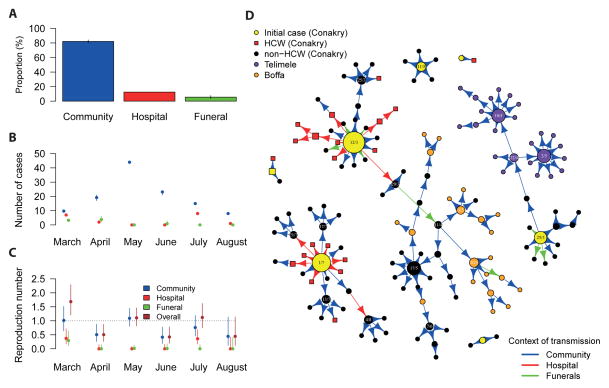
Between Feb 10, 2014, and Aug 25, 2014, we obtained data from the linelist of all confirmed and probable cases in Guinea (as of Sept 16, 2014), a laboratory database of information about patients, and interviews with patients and their families and neighbours. With this information, we mapped chains of transmission, identified which setting infections most probably originated from (community, hospitals, or funerals), and computed the context-specific and overall reproduction numbers.
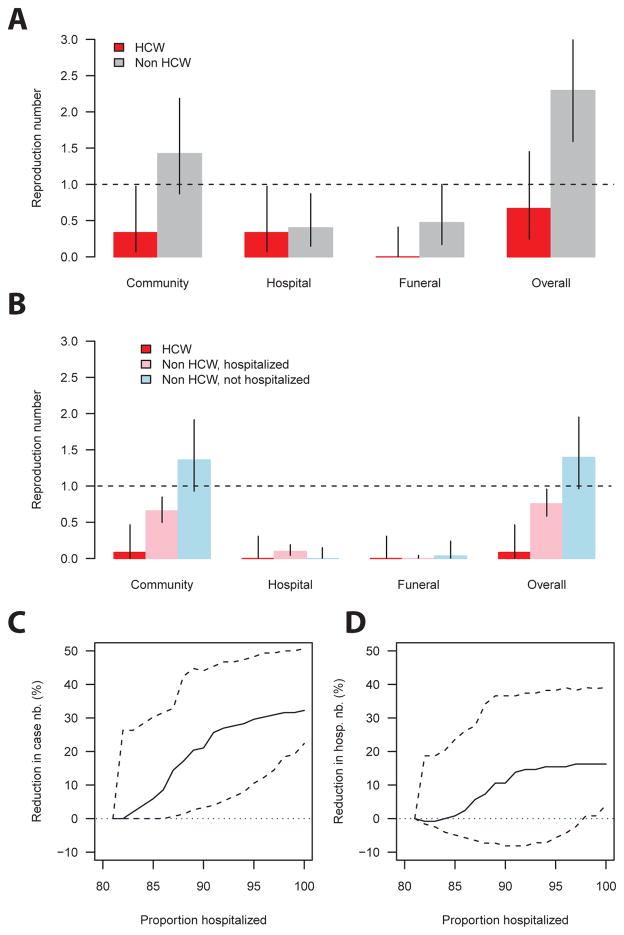
Of 193 confirmed and probable cases of Ebola virus disease reported in Conakry, Boffa, and Télimélé, 152 (79%) were positioned in chains of transmission. Health-care workers contributed little to transmission. In March, 2014, individuals with Ebola virus disease who were not health-care workers infected a mean of 2·3 people (95% CI 1·6-3·2): 1·4 (0·9-2·2) in the community, 0·4 (0·1-0·9) in hospitals, and 0·5 (0·2-1·0) at funerals. After the implementation of infection control in April, the reproduction number in hospitals and at funerals reduced to lower than 0·1. In the community, the reproduction number dropped by 50% for patients that were admitted to hospital, but remained unchanged for those that were not. In March, hospital transmissions constituted 35% (seven of 20) of all transmissions and funeral transmissions constituted 15% (three); but from April to the end of the study period, they constituted only 9% (11 of 128) and 4% (five), respectively. 82% (119 of 145) of transmission occurred in the community and 72% (105) between family members. Our simulations show that a 10% increase in hospital admissions could have reduced the length of chains by 26% (95% CI 4-45).
In Conakry, interventions had the potential to stop the epidemic, but reintroductions of the disease and poor cooperation of a few families led to prolonged low-level spread, showing the challenges of Ebola virus disease control in large urban centres. Monitoring of chains of transmission is crucial to assess and optimise local control strategies for Ebola virus disease.
Labex IBEID, Reacting, PREDEMICS, NIGMS MIDAS initiative, Institut Pasteur de Dakar.
埃博拉病毒病在西非部分地区持续爆发,规模空前。首次,科纳克里等大型城市中心也受到了影响。我们对几内亚三个地区(包括科纳克里)的埃博拉病毒病患者进行了观察性研究,旨在绘制传播链并评估干预措施的效果。
2014 年 2 月 10 日至 2014 年 8 月 25 日,我们从几内亚的确诊和可能病例列表中获取了数据(截至 2014 年 9 月 16 日)、一个有关患者信息的实验室数据库以及对患者及其家属和邻居的访谈。根据这些信息,我们绘制了传播链,确定了感染最有可能源自何处(社区、医院或葬礼),并计算了特定环境和总体繁殖数。
在报告的 193 例科纳克里、博法和泰利梅莱的埃博拉病毒病确诊和可能病例中,152 例(79%)位于传播链中。医务人员对传播的贡献很小。2014 年 3 月,非医务人员的埃博拉病毒病患者平均感染 2.3 人(95%CI 1.6-3.2):社区中 1.4(0.9-2.2)人,医院中 0.4(0.1-0.9)人,葬礼中 0.5(0.2-1.0)人。4 月实施感染控制后,医院和葬礼的繁殖数降至低于 0.1。在社区中,住院患者的繁殖数下降了 50%,但未住院患者的繁殖数没有变化。3 月,医院传播占所有传播的 35%(20 例中的 7 例),葬礼传播占 15%(3 例);但从 4 月到研究结束,它们分别仅占 9%(128 例中的 11 例)和 4%(5 例)。82%(145 例中的 119 例)的传播发生在社区,72%(105 例)发生在家庭成员之间。我们的模拟显示,住院人数增加 10%可能会使传播链减少 26%(95%CI 4-45)。
在科纳克里,干预措施有可能阻止疫情,但疾病的再次出现和少数家庭的合作不力导致疫情持续低水平传播,这表明在大型城市中心控制埃博拉病毒病具有挑战性。监测传播链对于评估和优化当地埃博拉病毒病控制策略至关重要。
IBEID 实验室、Reacting、PREDEMICS、NIGMS MIDAS 倡议、达喀尔巴斯德研究所。