Rizvi Rubina F, Harder Kathleen A, Hultman Gretchen M, Adam Terrence J, Kim Michael, Pakhomov Serguei V S, Melton Genevieve B
Institute for Health Informatics, University of Minnesota, Minneapolis, MN, United States.
Institute for Health Informatics, University of Minnesota, Minneapolis, MN, United States; Center for Design in Health, College of Design, University of Minnesota, Minneapolis, MN, United States.
Int J Med Inform. 2016 Jun;90:1-11. doi: 10.1016/j.ijmedinf.2016.02.011. Epub 2016 Mar 2.
The objective of this study is to understand physicians' usage of inpatient notes by (i) ascertaining different clinical note-entry and reading/retrieval styles in two different and widely used Electronic Health Record (EHR) systems, (ii) extrapolating potential factors leading to adoption of various note-entry and reading/retrieval styles and (iii) determining the amount of time to task associated with documenting different types of clinical notes.
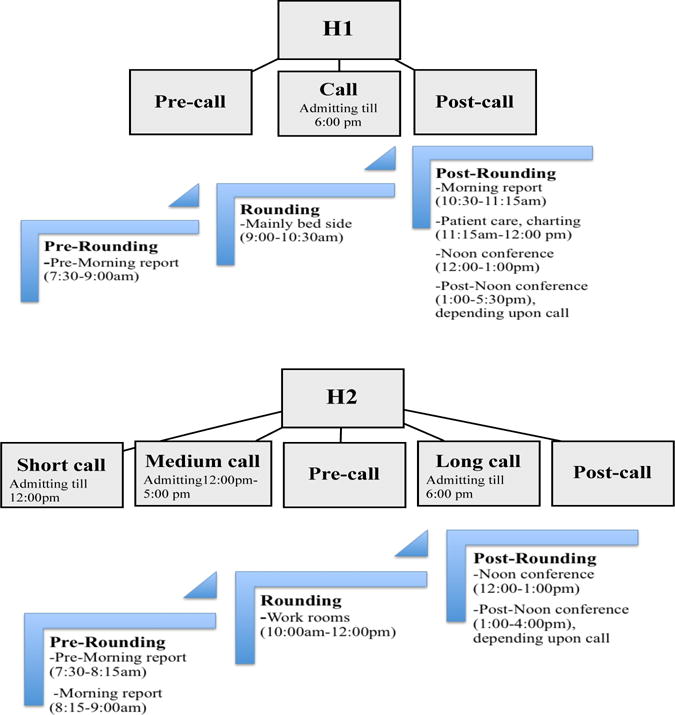
In order to answer "what" and "why" questions on physicians' adoption of certain-note-entry and reading/retrieval styles, an ethnographic study entailing Internal Medicine residents, with a mixed data analysis approach was performed. Participants were observed interacting with two different EHR systems in inpatient settings. Data was collected around the use and creation of History and Physical (H&P) notes, progress notes and discharge summaries.
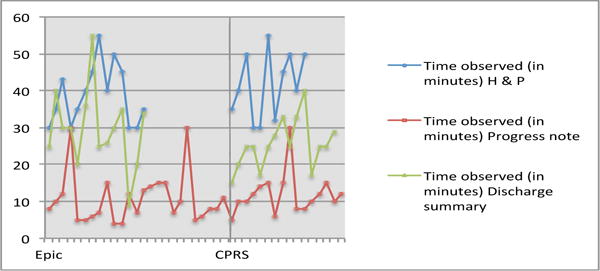
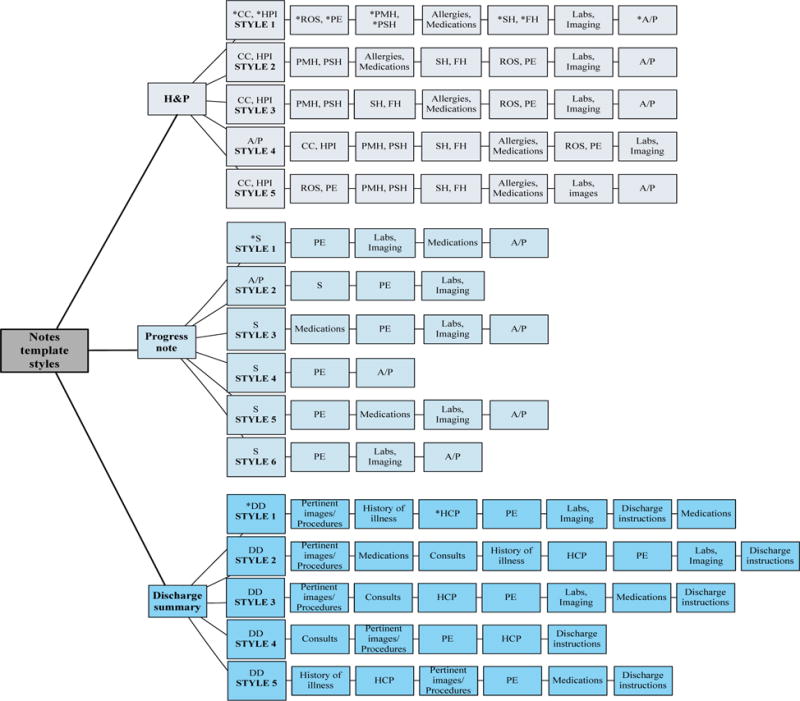
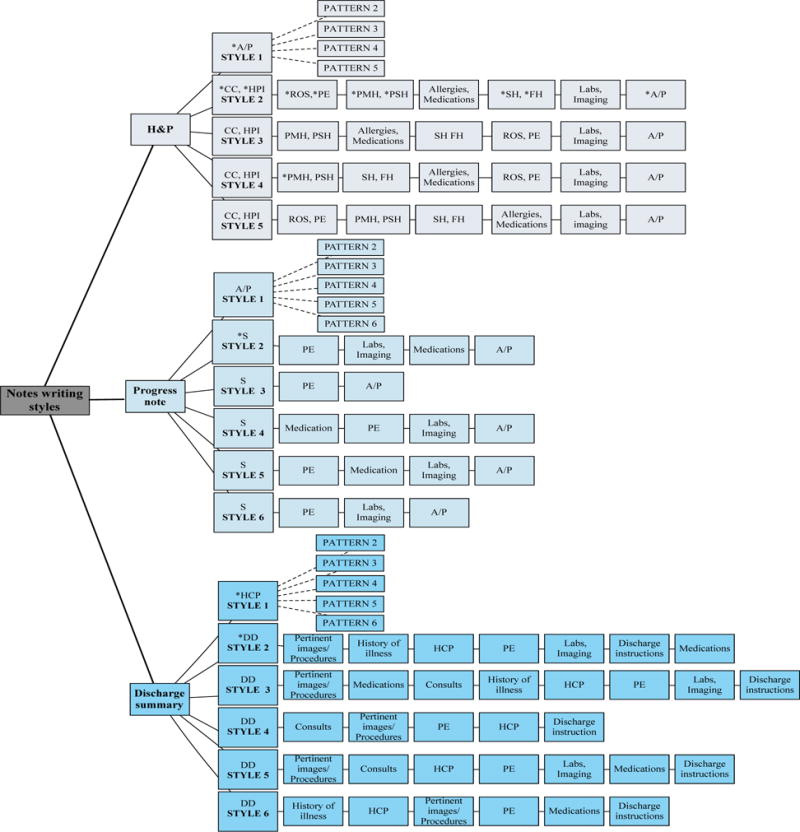
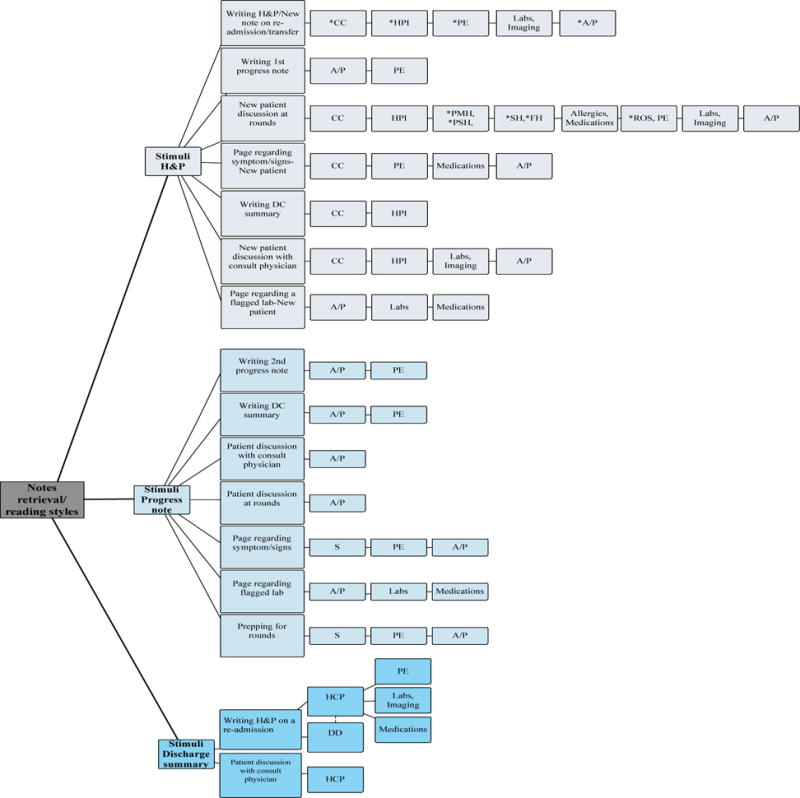
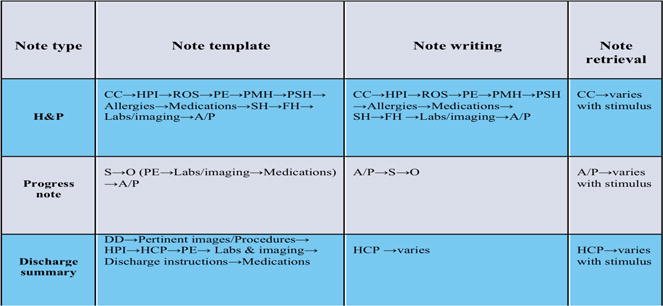
The highest variability in template styles was observed with progress notes and the least variability was within discharge summaries, while note-writing styles were most consistent for H&P notes. The first sections to be read in a H&P and progress note were the Chief Complaint and Assessment & Plan sections, respectively. The greatest note retrieval variability, with respect to the order of how note sections were reviewed, was observed with H&P and progress notes. Physician preference for adopting a certain reading/retrieval order appeared to be a function of what best fits their workflow while fulfilling the stimulus demands. The time spent entering H&P, discharge summaries and progress notes were similar in both EHRs.
This research study unveils existing variability in clinical documentation processes and provides us with important information that could help in designing a next generation EHR Graphical User Interface (GUI) that is more congruent with physicians' mental models, task performance needs, and workflow requirements.
本研究的目的是通过以下方式了解医生对住院病历的使用情况:(i)确定两种不同且广泛使用的电子健康记录(EHR)系统中的不同临床病历录入以及阅读/检索方式;(ii)推断导致采用各种病历录入以及阅读/检索方式的潜在因素;(iii)确定记录不同类型临床病历相关任务所花费的时间。
为了回答关于医生采用特定病历录入以及阅读/检索方式的“是什么”和“为什么”的问题,对内科住院医师进行了一项人种学研究,并采用了混合数据分析方法。观察参与者在住院环境中与两种不同的EHR系统进行交互的情况。收集了有关病史和体格检查(H&P)记录、病程记录和出院小结的使用和创建的数据。
病程记录的模板样式变化最大,出院小结的变化最小,而H&P记录的书写样式最为一致。在H&P记录和病程记录中,首先阅读的部分分别是主诉和评估与计划部分。在H&P记录和病程记录中,关于病历各部分审阅顺序的检索变化最大。医生对采用特定阅读/检索顺序的偏好似乎取决于最适合其工作流程同时满足刺激需求的因素。在两个EHR系统中,录入H&P记录、出院小结和病程记录所花费的时间相似。
本研究揭示了临床文档流程中存在的变异性,并为我们提供了重要信息,有助于设计与医生的心理模型、任务执行需求和工作流程要求更相符的下一代EHR图形用户界面(GUI)。