De Cock Erwin, Kritikou Persefoni, Sandoval Mariana, Tao Sunning, Wiesner Christof, Carella Angelo Michele, Ngoh Charles, Waterboer Tim
United Biosource Corporation, Barcelona, Spain.
United Biosource Corporation, London, United Kingdom.
PLoS One. 2016 Jun 30;11(6):e0157957. doi: 10.1371/journal.pone.0157957. eCollection 2016.
Rituximab is a standard treatment for non-Hodgkin lymphoma. The SABRINA trial (NCT01200758) showed that a subcutaneous (SC) rituximab formulation did not compromise efficacy or safety compared with intravenous (IV) infusion. We aimed to quantify active healthcare professional (HCP) time and patient chair time for rituximab SC and IV, including potential time savings.
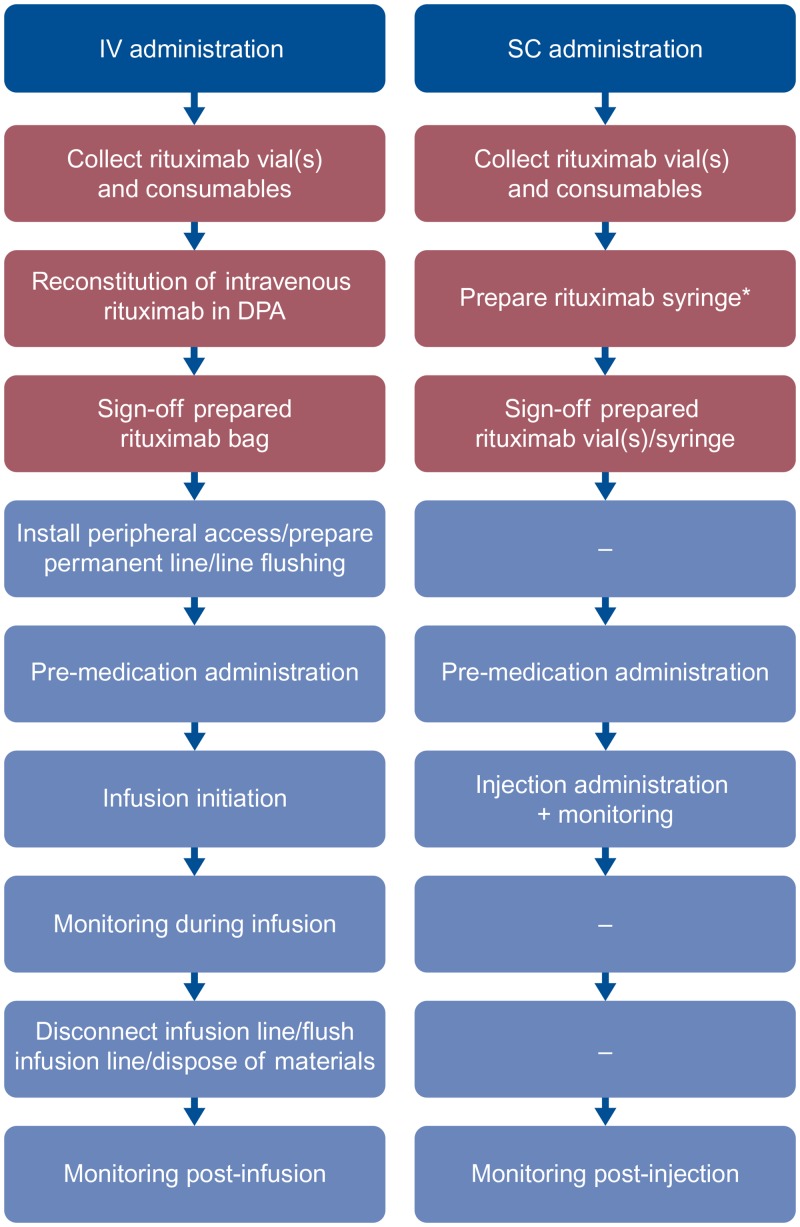
This non-interventional time and motion study was run in eight countries and 30 day oncology units. Rituximab SC data were collected alongside the MabCute trial (NCT01461928); IV data were collected per routine real-world practice. Trained observers recorded active HCP time for pre-specified tasks (stopwatch) and chair time (time of day). A random intercept model was used to analyze active HCP time (by task and for all tasks combined) in the treatment room and drug preparation area, drug administration duration, chair time and patient treatment room time by country and/or across countries. Active HCP and chair time were extrapolated to a patient's first year of treatment (11 rituximab sessions).
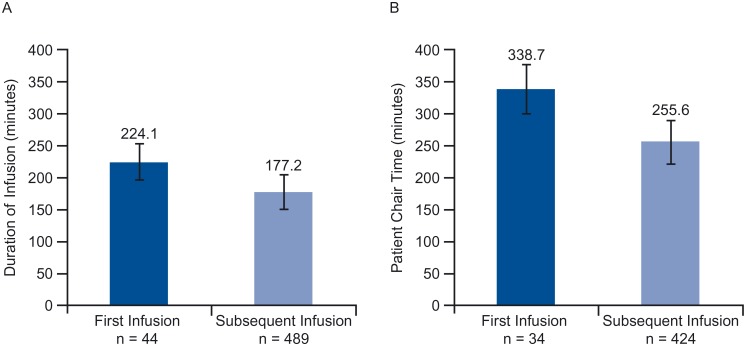
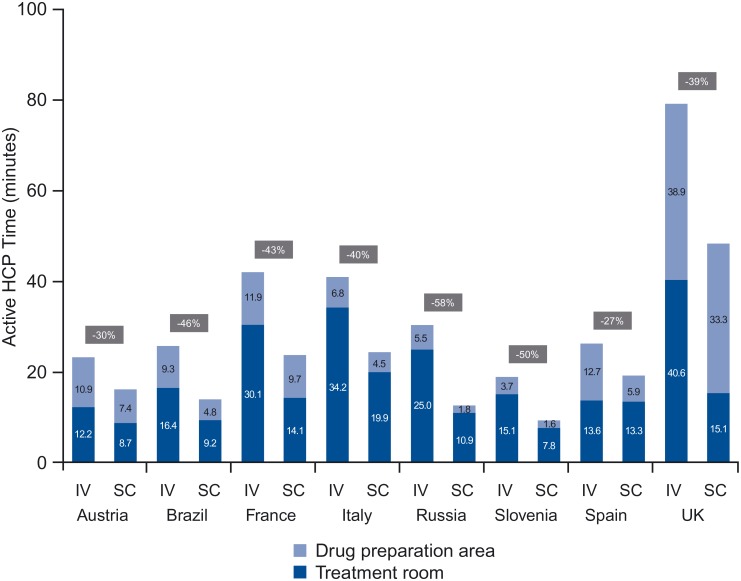
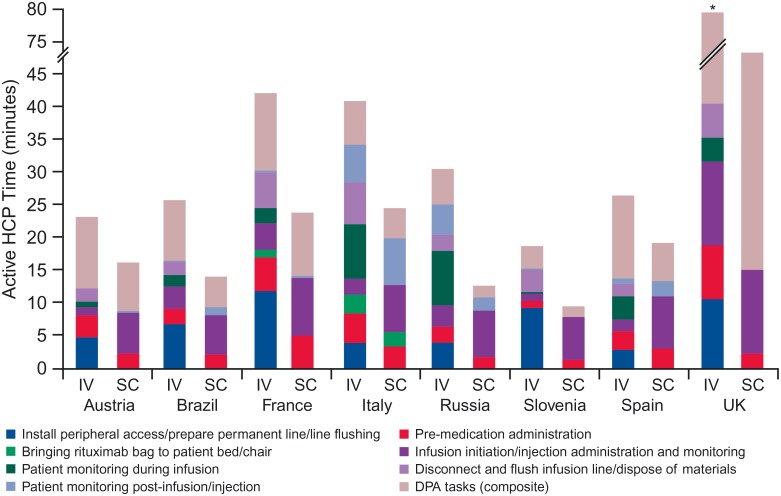
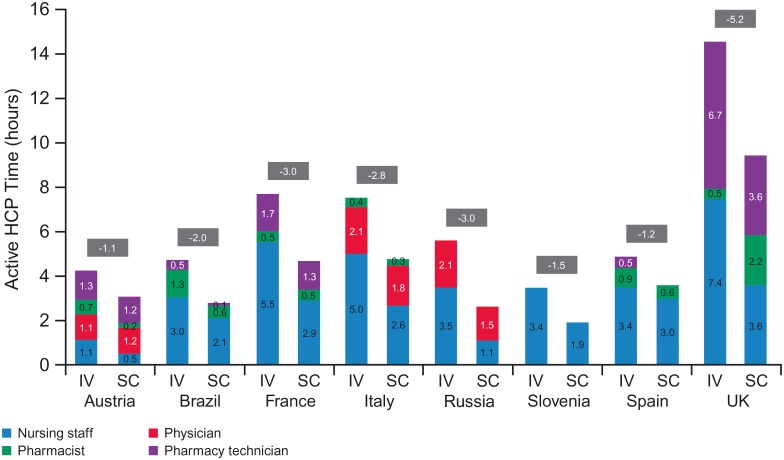
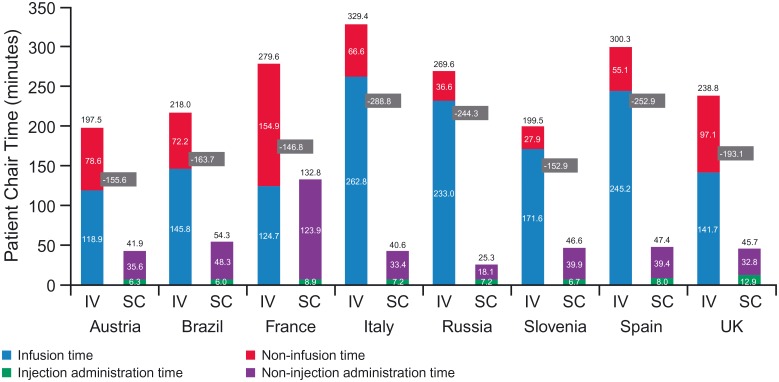
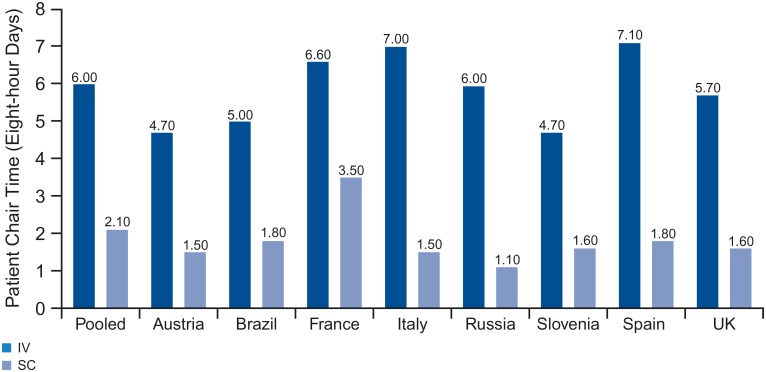
Mean active HCP time was 35.0 and 23.7 minutes for IV and SC process, respectively (-32%, p <0.0001). By country, relative reduction in time was 27-58%. Absolute reduction in extrapolated active HCP time (first year of treatment) was 1.1-5.2 hours. Mean chair time was 262.1 minutes for IV, including 180.9 minutes infusion duration, vs. 67.3 minutes for SC, including 8.3 minutes SC injection administration (-74%, p <0.0001). By country, relative reduction was 53-91%. Absolute reduction in extrapolated chair time for the first year of treatment was 3.1-5.5 eight-hour days.
Compared with rituximab IV, rituximab SC was associated with reduced chair time and active HCP time. The latter could be invested in other activities, whereas the former may lead to more available appointments, reducing waiting lists and increasing the efficiency of day oncology units.
ClinicalTrials.gov NCT01200758.
利妥昔单抗是治疗非霍奇金淋巴瘤的标准疗法。SABRINA试验(NCT01200758)表明,皮下注射(SC)利妥昔单抗制剂与静脉输注(IV)相比,疗效和安全性并未降低。我们旨在量化医疗保健专业人员(HCP)使用利妥昔单抗SC和IV的实际工作时间以及患者的候诊时间,包括潜在的时间节省情况。
这项非干预性的时间与动作研究在8个国家的30个肿瘤科室开展。利妥昔单抗SC的数据是在MabCute试验(NCT01461928)期间收集的;IV的数据则按照常规实际操作进行收集。经过培训的观察员记录完成预先指定任务的HCP实际工作时间(使用秒表)和候诊时间(一天中的时间)。采用随机截距模型分析不同国家和/或所有国家汇总后,治疗室和药物准备区域内HCP的实际工作时间(按任务和所有任务汇总)、给药持续时间、候诊时间以及患者在治疗室的时间。HCP的实际工作时间和候诊时间外推至患者治疗的第一年(11次利妥昔单抗治疗疗程)。
IV和SC治疗过程中,HCP的平均实际工作时间分别为35.0分钟和23.7分钟(减少32%,p<0.0001)。按国家来看,时间相对减少了27%-58%。外推至治疗第一年的HCP实际工作时间绝对减少了1.