Landi Francesco, Calvani Riccardo, Tosato Matteo, Martone Anna Maria, Bernabei Roberto, Onder Graziano, Marzetti Emanuele
Department of Geriatrics, Neurosciences and Orthopaedics, Catholic University of the Sacred Heart, Rome, Italy.
BMJ Open. 2016 Jul 25;6(7):e008281. doi: 10.1136/bmjopen-2015-008281.
Sarcopaenia and physical function impairment may have a greater effect on survival than other clinical characteristics, including multimorbidity. In this study, we evaluated the impact of sarcopaenia on all-cause mortality and the interaction among muscle loss, physical function impairment and multimorbidity on mortality risk over 10 years in older community-dwellers.
Prospective cohort study.
Population-based study.
All persons aged 80+ years living in the community in the Sirente geographic area (L'Aquila, Italy) (n=364). Participants were categorised in the sarcopaenic or non-sarcopaenic group based on the European Working Group on Sarcopenia in Older People criteria.
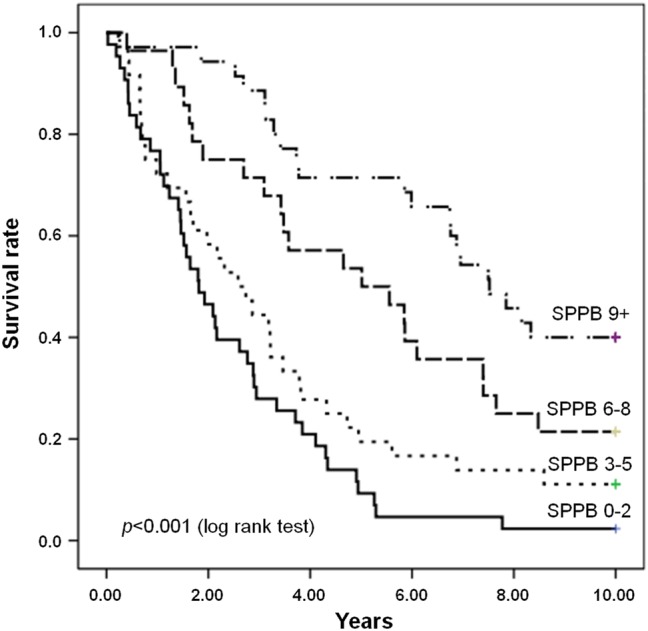
(1) All-cause mortality over 10 years according to the presence of sarcopaenia and (2) impact of physical function impairment, assessed using the Short Physical Performance Battery (SPPB), and multimorbidity on 10-year mortality risk in persons with sarcopaenia.
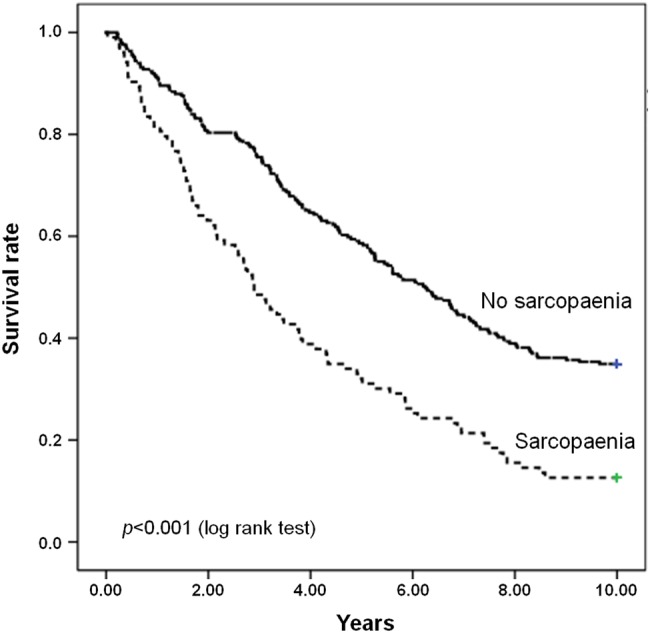
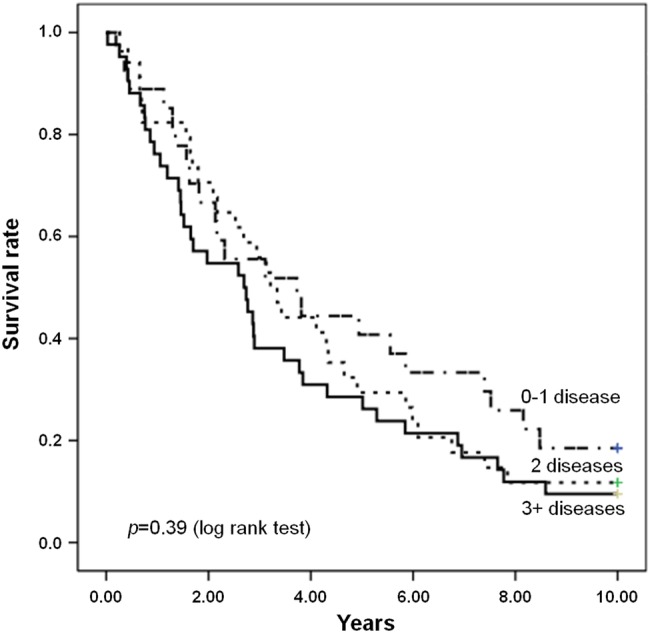
Sarcopaenia was identified in 103 participants (29.1%). A total of 253 deaths were recorded over 10 years: 90 among sarcopaenic participants (87.4%) and 162 among non-sarcopaenic persons (65.1%; p<0.001). Participants with sarcopaenia had a higher risk of death than those without sarcopaenia (HR=2.15; 95% CI 1.02 to 4.54). When examining the effect of sarcopaenia and physical function impairment on mortality, participants with low physical performance levels showed greater mortality. Conversely, the mortality risk was unaffected by multimorbidity.
Our findings show that physical function impairment, but not multimorbidity, is predictive of mortality in older community-dwellers with sarcopaenia. Hence, in sarcopaenic older persons, interventions against functional decline may be more effective at preventing or postponing negative health outcomes than those targeting multimorbidity.
与包括多种疾病并存在内的其他临床特征相比,肌肉减少症和身体功能损害对生存的影响可能更大。在本研究中,我们评估了肌肉减少症对全因死亡率的影响,以及肌肉量减少、身体功能损害和多种疾病并存之间的相互作用对老年社区居民10年死亡风险的影响。
前瞻性队列研究。
基于人群的研究。
居住在意大利拉奎拉省锡伦特地理区域社区的所有80岁及以上老人(n = 364)。根据欧洲老年人肌肉减少症工作组的标准将参与者分为肌肉减少症组或非肌肉减少症组。
(1)根据是否存在肌肉减少症评估10年全因死亡率;(2)使用简短体能状况量表(SPPB)评估身体功能损害以及多种疾病并存对肌肉减少症患者10年死亡风险的影响。
103名参与者(29.1%)被确定患有肌肉减少症。10年间共记录了253例死亡:肌肉减少症参与者中有90例(87.4%),非肌肉减少症者中有162例(65.1%;p<0.001)。肌肉减少症参与者的死亡风险高于非肌肉减少症参与者(HR = 2.15;95%CI 1.02至4.54)。在研究肌肉减少症和身体功能损害对死亡率的影响时,身体表现水平低的参与者死亡率更高。相反,多种疾病并存对死亡风险没有影响。
我们的研究结果表明,身体功能损害而非多种疾病并存可预测患有肌肉减少症的老年社区居民的死亡率。因此,对于患有肌肉减少症的老年人,针对功能衰退的干预措施在预防或推迟不良健康结局方面可能比针对多种疾病并存的干预措施更有效。