Kallela Jenni, Jääskeläinen Tiina, Kortelainen Eija, Heinonen Seppo, Kajantie Eero, Kere Juha, Kivinen Katja, Pouta Anneli, Laivuori Hannele
Medical and Clinical Genetics, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
Obstetrics and Gynaecology, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
BMC Pregnancy Childbirth. 2016 Aug 12;16:221. doi: 10.1186/s12884-016-1010-0.
The Finnish Pre-eclampsia Consortium (FINNPEC) case-control cohort consisting of 1447 pre-eclamptic and 1068 non-pre-eclamptic women was recruited during 2008-2011 to study genetic background of pre-eclampsia and foetal growth. Pre-eclampsia was defined by hypertension and proteinuria according to the American College of Obstetricians and Gynecologists (ACOG) 2002 classification. The ACOG Task Force Report on Hypertension in Pregnancy (2013) and The International Society for the Study of Hypertension in Pregnancy (ISSHP) (2014) have published new classifications, in which proteinuria is not necessary for diagnosis when specific symptoms are present. For diagnoses based on proteinuria, the ISSHP 2014 criteria raised its threshold to 2+ on dipstick. We studied how the new classifications would affect pre-eclampsia diagnoses in the FINNPEC cohort.
We re-evaluated pre-eclampsia diagnosis using the ACOG 2013 and the ISSHP 2014 classifications in pre-eclamptic women whose proteinuria did not exceed 1+ on dipstick (n = 68), in women with gestational hypertension (n = 138) and in women with chronic hypertension (n = 66).
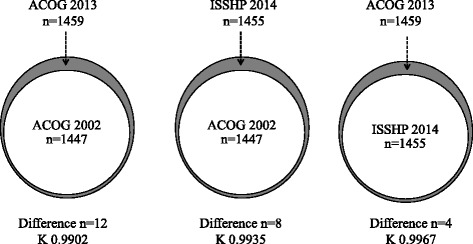
The number of women with pre-eclampsia increased 0.8 % (1459/1447) according to the ACOG 2013 criteria and 0.6 % (1455/1447) according to the ISSHP 2014 criteria. All 68 women with the amount of proteinuria not exceeding 1+ on dipstick diagnosed originally pre-eclamptic met the ACOG 2013 criteria but only 20 women (29.4 %) met the ISSHP 2014 criteria. Seven (5.1 %) and 35 (25.4 %) women with gestational hypertension were diagnosed with pre-eclampsia according to the ACOG 2013 and the ISSHP 2014 criteria, respectively. Correspondingly five (7.6 %) and 21 (31.8 %) women with chronic hypertension were diagnosed with pre-eclampsia according to the ACOG 2 013 and the ISSHP 2014 criteria.
Only minor changes were observed in the total number of pre-eclamptic women in the FINNPEC cohort when comparing the ACOC 2002 classification with the ACOG 2013 and ISSHP 2014 classifications.
芬兰子痫前期联盟(FINNPEC)病例对照队列由1447例子痫前期妇女和1068例非子痫前期妇女组成,于2008年至2011年招募,用于研究子痫前期和胎儿生长的遗传背景。根据美国妇产科医师学会(ACOG)2002年分类,子痫前期由高血压和蛋白尿定义。ACOG关于妊娠期高血压的特别工作组报告(2013年)和国际妊娠高血压研究学会(ISSHP)(2014年)发布了新的分类,其中当出现特定症状时,蛋白尿并非诊断必需条件。对于基于蛋白尿的诊断,ISSHP 2014年标准将试纸条检测阈值提高到2+。我们研究了新分类如何影响FINNPEC队列中的子痫前期诊断。
我们使用ACOG 2013年和ISSHP 2014年分类重新评估了蛋白尿试纸条检测不超过1+的子痫前期妇女(n = 68)、妊娠期高血压妇女(n = 138)和慢性高血压妇女(n = 66)的子痫前期诊断。
根据ACOG 2013年标准,子痫前期妇女数量增加了0.8%(1459/1447),根据ISSHP 2014年标准增加了0.6%(1455/1447)。最初诊断为子痫前期的所有68例蛋白尿试纸条检测不超过1+的妇女均符合ACOG 2013年标准,但只有20例妇女(29.4%)符合ISSHP 2014年标准。根据ACOG 2013年和ISSHP 2014年标准,分别有7例(5.1%)和35例(25.4%)妊娠期高血压妇女被诊断为子痫前期。相应地,根据ACOG 2013年和ISSHP 2014年标准,分别有5例(7.6%)和21例(31.8%)慢性高血压妇女被诊断为子痫前期。
将ACOG 2002年分类与ACOG 2013年和ISSHP 2014年分类进行比较时,FINNPEC队列中子痫前期妇女总数仅出现了微小变化。