Key Laboratory of Respiratory Disease of Zhejiang Province, Department of Respiratory and Critical Care Medicine, Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People's Republic of China.
Department of Respiratory and Critical Care Medicine, Haining People's Hospital, Haining Branch, The First Affiliated Hospital, Zhejiang University, Haining, Zhejiang, People's Republic of China.
Int J Chron Obstruct Pulmon Dis. 2021 Dec 30;16:3551-3559. doi: 10.2147/COPD.S347948. eCollection 2021.
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) could be triggered by community-acquired pneumonia (CAP). Peripheral blood eosinopenia are strongly associated with increased mortality. In hospitalized AECOPD patients with CAP, eosinopenia may be used to identify patients with high risk of death on admission.
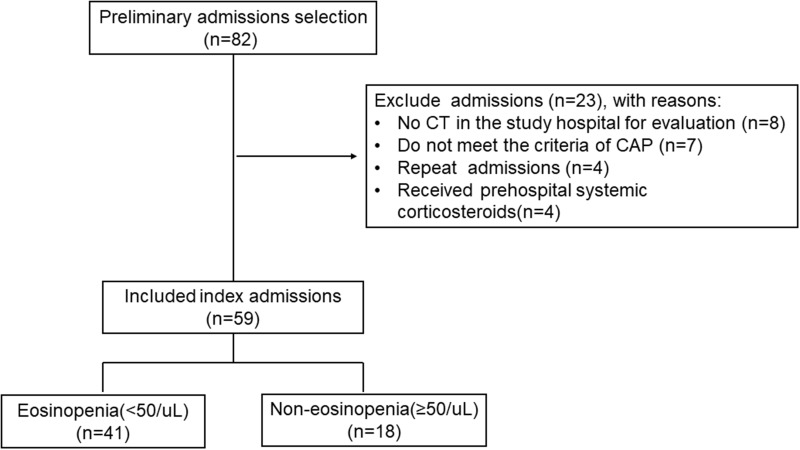
We conducted a retrospective cohort study in 82 hospitalized AECOPD patients with CAP. Patients who had received systemic corticosteroids preadmission were excluded. The patients were identified by individual case file review. According to blood eosinophil count, patients were grouped as eosinopenia (<50/μL) and non-eosinopenia (≥50/μL). Association of eosinopenia with infection and 18-month survival were analyzed using appropriate statistical methods.
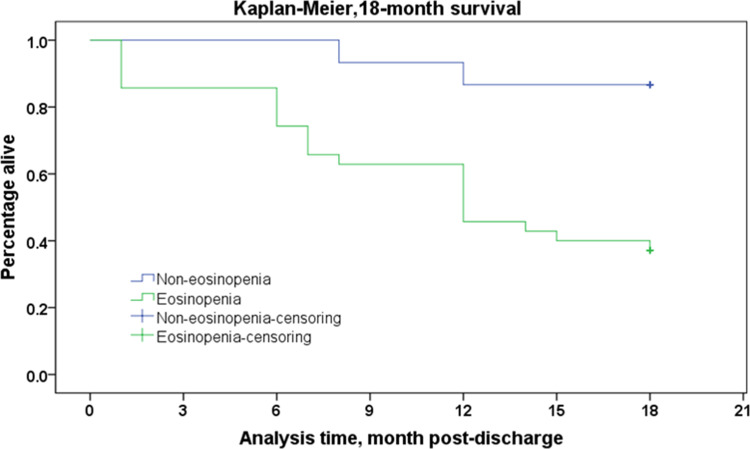
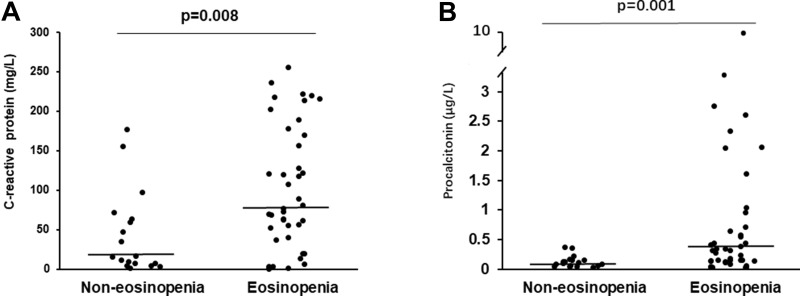
Baseline demographic, comorbidity, CURB65 and Pneumonia Severity Index scores were similar between two groups. The eosinopenia group had significantly higher pro-brain natriuretic peptide, D-dimer, neutrophil percentage, and lower lymphocyte count and lymphocyte percentage. The eosinopenia group had significantly higher C-reactive protein (median 77.30 vs 16.55, =0.008) and procalcitonin (median 0.32 vs 0.12, =0.001). Survival at 18 months after hospital discharge was significantly lower in the eosinopenia group vs non-eosinopenia group (log rank, =0.002).
Eosinopenia (<50/μL) was a strong predictor of 18-month mortality and associated with more severe infection in hospitalized AECOPD patients with CAP. Eosinophil count at admission can be used as a prognosis marker of mortality in those population.
慢性阻塞性肺疾病(COPD)急性加重(AECOPD)可由社区获得性肺炎(CAP)引发。外周血嗜酸性粒细胞减少与死亡率增加密切相关。在患有 CAP 的住院 AECOPD 患者中,嗜酸性粒细胞减少可能用于识别入院时死亡风险较高的患者。
我们对 82 例患有 CAP 的住院 AECOPD 患者进行了回顾性队列研究。排除了入院前接受全身皮质类固醇治疗的患者。通过个案文件回顾确定患者。根据血嗜酸性粒细胞计数,将患者分为嗜酸性粒细胞减少症(<50/μL)和非嗜酸性粒细胞减少症(≥50/μL)。采用适当的统计方法分析嗜酸性粒细胞减少与感染和 18 个月生存率的关系。
两组患者的基线人口统计学、合并症、CURB65 和肺炎严重指数评分相似。嗜酸性粒细胞减少组的脑钠肽前体、D-二聚体、中性粒细胞百分比明显升高,淋巴细胞计数和淋巴细胞百分比明显降低。嗜酸性粒细胞减少组的 C 反应蛋白(中位数 77.30 与 16.55,=0.008)和降钙素原(中位数 0.32 与 0.12,=0.001)明显升高。出院后 18 个月的生存率在嗜酸性粒细胞减少组明显低于非嗜酸性粒细胞减少组(对数秩检验,=0.002)。
嗜酸性粒细胞减少症(<50/μL)是预测 18 个月死亡率的有力指标,与患有 CAP 的住院 AECOPD 患者更严重的感染相关。入院时的嗜酸性粒细胞计数可作为该人群死亡率的预后标志物。