Nassiri Nima, Margolis Daniel J, Natarajan Shyam, Sharma Devi S, Huang Jiaoti, Dorey Frederick J, Marks Leonard S
Department of Urology (NN, SN, DSS, LSM), University of California-Los Angeles, Los Angeles, California; Department of Radiology (DJM), University of California-Los Angeles, Los Angeles, California; Department of Biomedical Engineering (SN), University of California-Los Angeles, Los Angeles, California; Department of Pathology, Duke University School of Medicine (JH), Durham, North Carolina.
Department of Urology (NN, SN, DSS, LSM), University of California-Los Angeles, Los Angeles, California; Department of Radiology (DJM), University of California-Los Angeles, Los Angeles, California; Department of Biomedical Engineering (SN), University of California-Los Angeles, Los Angeles, California; Department of Pathology, Duke University School of Medicine (JH), Durham, North Carolina.
J Urol. 2017 Mar;197(3 Pt 1):632-639. doi: 10.1016/j.juro.2016.09.070. Epub 2016 Sep 14.
We sought to determine the rate of upgrading to Gleason score 4 + 3 or greater using targeted biopsy for diagnosis and monitoring in men undergoing active surveillance of prostate cancer.
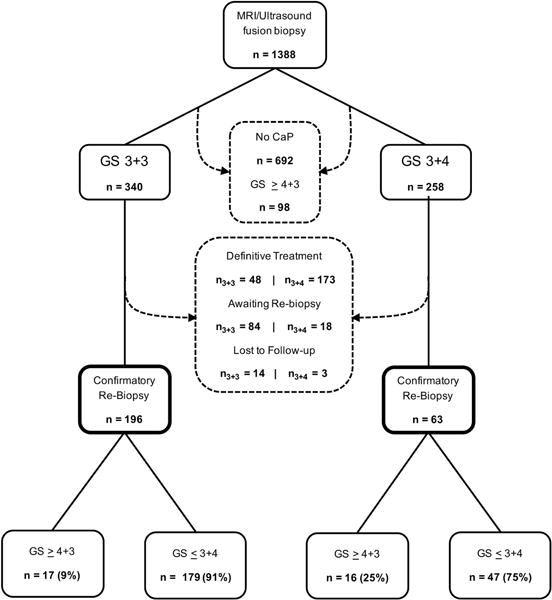
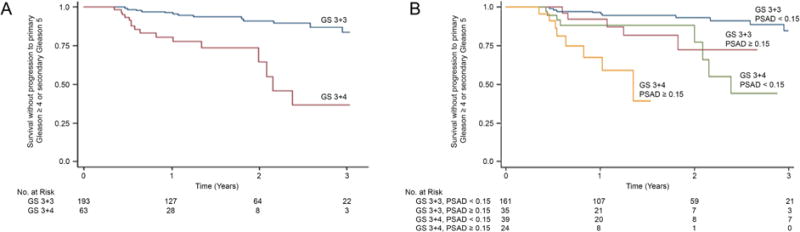
Study subjects comprised all 259 men, including 196 with Gleason score 3 + 3 and 63 with Gleason score 3 + 4, who were diagnosed by magnetic resonance imaging/ultrasound fusion guided biopsy from 2009 to 2015 and underwent subsequent fusion biopsy for as long as 4 years of active surveillance. The primary end point was the discovery of Gleason score 4 + 3 or greater prostate cancer. Followup biopsies included targeting of positive sites, which were tracked in an Artemis™ device. Kaplan-Meier curves were generated to determine upgrading rates, stratified by initial Gleason score and prostate specific antigen density.
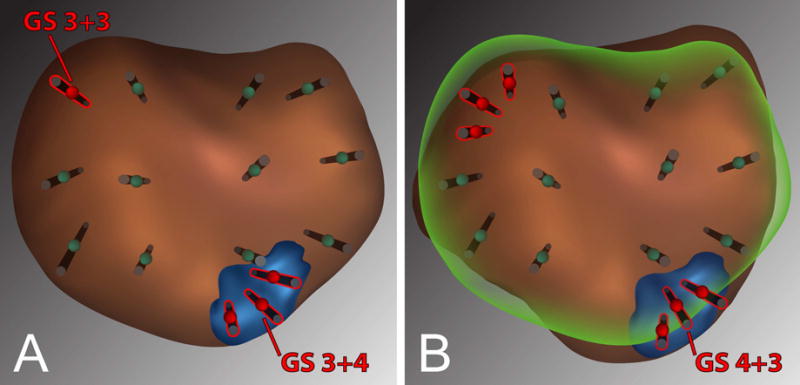
Based on a Cox proportional hazard model, men with Gleason score 3 + 4 were 4.65 times more likely to have upgrading than men with an initial Gleason score of 3 + 3 at 3 years (p <0.01). By the third surveillance year 63% of men with Gleason score 3 + 4 had been upgraded compared with 18.0% who started with Gleason score 3 + 3 (p <0.01). Of all 33 upgrades 32 (97%) occurred at a magnetic resonance imaging visible or a tracked site of tumor, rather than at a previously negative systematic site. Independent predictors of upgrading were Gleason score 3 + 4, prostate specific antigen density 0.15 ng/ml/cm or greater and a grade 5 lesion on magnetic resonance imaging. The incidence rate ratio of upgrading (Gleason score 3 + 4 vs 3 + 3) was 4.25 per year of patient followup (p <0.01).
During active surveillance of prostate cancer, targeting of tracked tumor foci by magnetic resonance imaging/ultrasound fusion biopsy allows for heightened detection of Gleason score 4 + 3 or greater cancers. Baseline variables directly related to important upgrading that warrant increased vigilance include Gleason score 3 + 4, prostate specific antigen density 0.15 ng/ml/cm or greater and grade 5 lesions on magnetic resonance imaging.
我们试图确定在接受前列腺癌主动监测的男性中,使用靶向活检进行诊断和监测时,升级为Gleason评分4+3或更高的比例。
研究对象包括2009年至2015年通过磁共振成像/超声融合引导活检确诊的所有259名男性,其中196名Gleason评分为3+3,63名Gleason评分为3+4,并在长达4年的主动监测期间接受了后续融合活检。主要终点是发现Gleason评分4+3或更高的前列腺癌。随访活检包括对阳性部位进行靶向活检,这些部位在Artemis™设备中进行跟踪。生成Kaplan-Meier曲线以确定升级率,并按初始Gleason评分和前列腺特异性抗原密度进行分层。
基于Cox比例风险模型,在3年时,Gleason评分为3+4的男性升级的可能性是初始Gleason评分为3+3的男性的4.65倍(p<0.01)。到第三个监测年,63%的Gleason评分为3+4的男性发生了升级,而初始Gleason评分为3+3的男性中这一比例为18.0%(p<0.01)。在所有33例升级病例中,32例(97%)发生在磁共振成像可见或跟踪的肿瘤部位,而不是在先前为阴性的系统部位。升级的独立预测因素包括Gleason评分为3+4、前列腺特异性抗原密度为0.15 ng/ml/cm或更高以及磁共振成像上的5级病变。患者随访每年升级的发病率比(Gleason评分3+4与3+3相比)为4.25(p<0.01)。
在前列腺癌主动监测期间,通过磁共振成像/超声融合活检对跟踪的肿瘤病灶进行靶向活检,能够提高对Gleason评分4+3或更高癌症的检测率。与重要升级直接相关且需要提高警惕的基线变量包括Gleason评分为3+4、前列腺特异性抗原密度为0.15 ng/ml/cm或更高以及磁共振成像上的5级病变。