Agyepong Irene Akua, Abankwah Daniel Nana Yaw, Abroso Angela, Chun ChangBae, Dodoo Joseph Nii Otoe, Lee Shinye, Mensah Sylvester A, Musah Mariam, Twum Adwoa, Oh Juwhan, Park Jinha, Yang DoogHoon, Yoon Kijong, Otoo Nathaniel, Asenso-Boadi Francis
Ghana Health Service, Research and Development Division, P.O. Box 1, Dodowa, Greater Accra Region, Ghana.
Department of Social and Behavioral Sciences, University of Ghana, School of Public Health, Accra, Ghana.
BMC Health Serv Res. 2016 Sep 21;16(1):504. doi: 10.1186/s12913-016-1758-y.
Despite universal population coverage and equity being a stated policy goal of its NHIS, over a decade since passage of the first law in 2003, Ghana continues to struggle with how to attain it. The predominantly (about 70 %) tax funded NHIS currently has active enrolment hovering around 40 % of the population. This study explored in-depth enablers and barriers to enrolment in the NHIS to provide lessons and insights for Ghana and other low and middle income countries (LMIC) into attaining the goal of universality in Universal Health Coverage (UHC).
We conducted a cross sectional mixed methods study of an urban and a rural district in one region of Southern Ghana. Data came from document review, analysis of routine data on enrolment, key informant in-depth interviews with local government, regional and district insurance scheme and provider staff and community member in-depth interviews and focus group discussions.
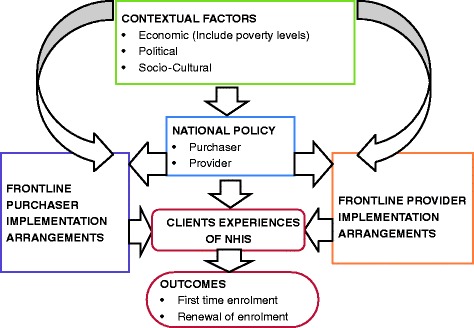
Population coverage in the NHIS in the study districts was not growing towards near universal because of failure of many of those who had ever enrolled to regularly renew annually as required by the NHIS policy. Factors facilitating and enabling enrolment were driven by the design details of the scheme that emanate from national level policy and program formulation, frontline purchaser and provider staff implementation arrangements and contextual factors. The factors inter-related and worked together to affect client experience of the scheme, which were not always the same as the declared policy intent. This then also affected the decision to enrol and stay enrolled.
UHC policy and program design needs to be such that enrolment is effectively compulsory in practice. It also requires careful attention and responsiveness to actual and potential subscriber, purchaser and provider (stakeholder) incentives and related behaviour generated at implementation levels.
尽管全民覆盖和平等是加纳国家健康保险计划(NHIS)宣称的政策目标,但自2003年第一部相关法律通过后的十多年里,加纳仍在努力探索如何实现这一目标。主要由税收资助(约70%)的NHIS目前的有效参保人数徘徊在总人口的40%左右。本研究深入探讨了NHIS参保的促进因素和障碍,为加纳及其他低收入和中等收入国家(LMIC)实现全民健康覆盖(UHC)的普遍性目标提供经验教训和见解。
我们在加纳南部一个地区的一个城市和一个农村地区进行了一项横断面混合方法研究。数据来自文件审查、参保常规数据分析、对地方政府、地区和区级保险计划及提供者工作人员的关键信息提供者深入访谈,以及社区成员深入访谈和焦点小组讨论。
研究地区NHIS的人口覆盖率并未朝着接近全民覆盖的方向增长,原因是许多曾经参保的人未能按照NHIS政策要求每年定期续保。促进参保的因素由国家层面政策和计划制定产生的计划设计细节、一线购买者和提供者工作人员的实施安排以及背景因素驱动。这些因素相互关联并共同作用,影响了客户对该计划的体验,而这种体验并不总是与宣称的政策意图一致。这进而也影响了参保和持续参保的决定。
UHC政策和计划设计应确保在实际中有效强制参保。它还需要仔细关注并回应实际和潜在参保者、购买者和提供者(利益相关者)在实施层面产生的激励措施及相关行为。