Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine, Beijing Chao-Yang Hospital Beijing, Capital Medical University, No, 8 Gong Ti Southern Road, Chao Yang District, Beijing 100020, China.
Eur J Med Res. 2014 Apr 8;19(1):18. doi: 10.1186/2047-783X-19-18.
Exacerbations of chronic obstructive pulmonary disease (COPD) are sporadic, acute worsening of symptoms. Identifying predictors of exacerbation frequency may facilitate medical interventions that reduce exacerbation frequency and severity. The objective of this study was to determine predictors of exacerbation frequency and mortality.
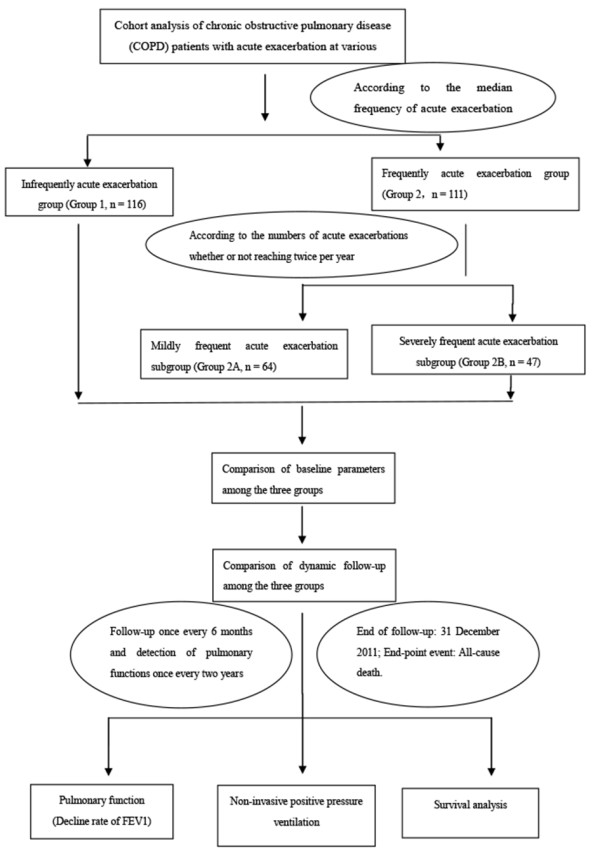
A total of 227 COPD patients were enrolled in a prospective clinical study between January 2000 and December 2011. Reported exacerbations were recorded for the year preceding enrollment and annually thereafter, and patients were grouped by median annual exacerbation frequency into those experiencing infrequent exacerbations (less than one exacerbation annually) and frequent exacerbations (one or more exacerbation annually). Patients experiencing frequent exacerbations were further divided into those experiencing moderately frequent exacerbations (fewer than two exacerbations per year) and severely frequent exacerbations (two or more exacerbations per year). The rate of clinical relapse and survival was recorded over a 10-year period. The mean of follow-up time was 5.15 years per patient.
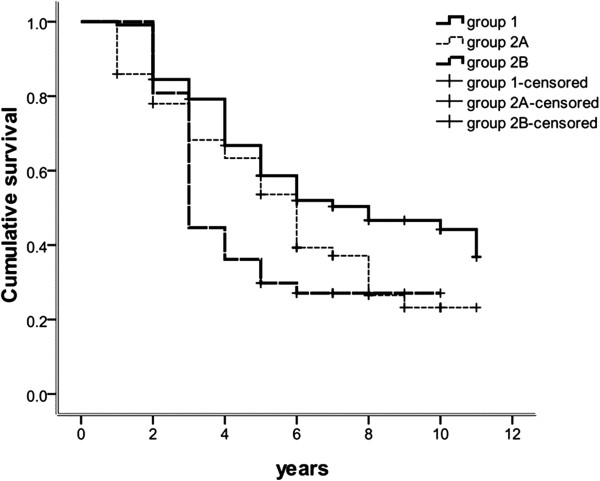
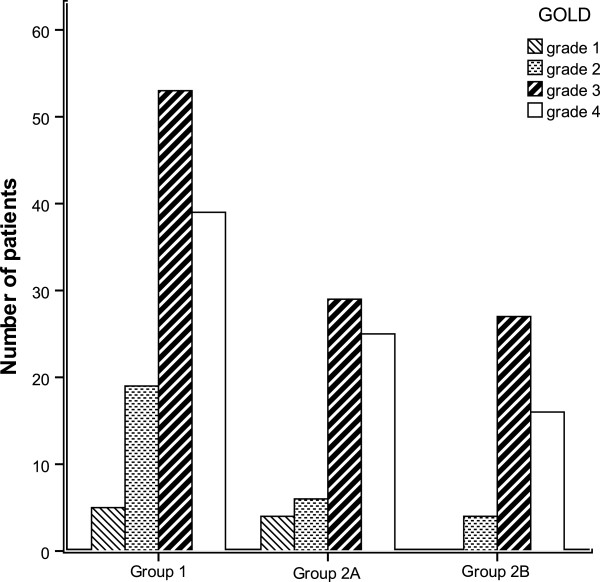
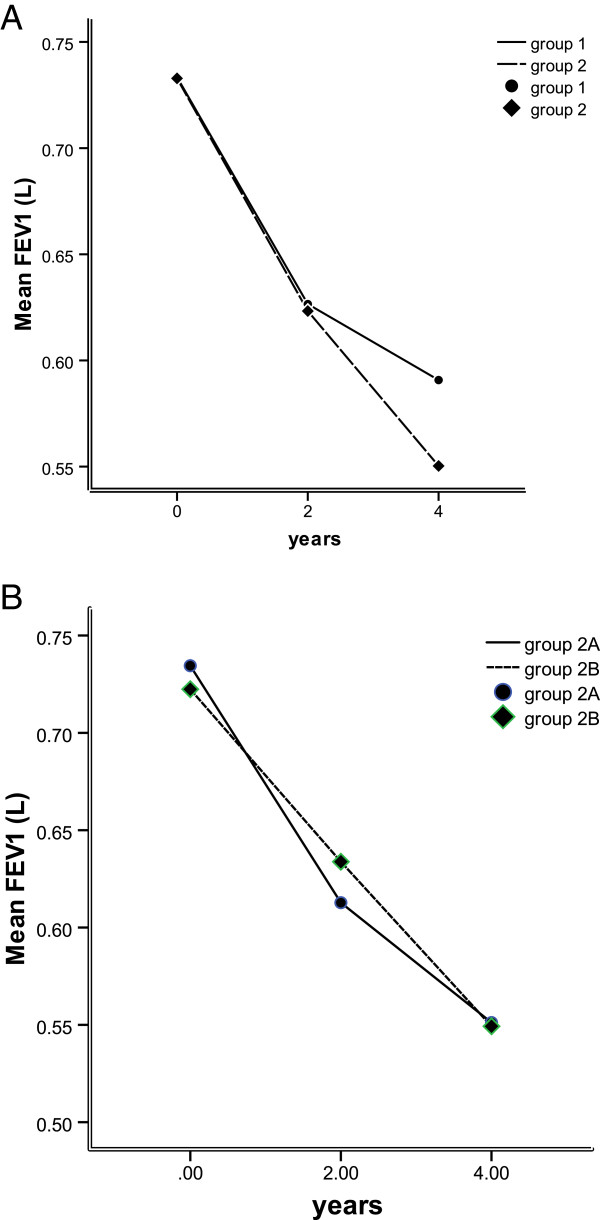
For patients experiencing infrequent, moderately frequent, and severely frequent exacerbations, median exacerbations in the year preceding enrollment were 0.0, 0.5, 1.0, respectively, and more frequent exacerbations correlated with lower baseline forced expiratory volume in one second (FEV1) (0.81 L, 0.75 L, and 0.66 L, respectively), higher comorbidity (70.7%, 75.0%, and 89.4%, respectively), and greater NPPV use during hospitalization (16.4%, 35.9% and 51.1%, respectively). FEV1 declined and mortality increased with increasing exacerbation frequency.
Exacerbation frequency can be used to generate discreet patient subpopulations, supporting the hypothesis that multiple COPD phenotypes exist and can be used in patient risk stratification.
慢性阻塞性肺疾病(COPD)的加重是指症状的偶发性、急性恶化。确定加重频率的预测因素可以促进减少加重频率和严重程度的医疗干预。本研究的目的是确定加重频率和死亡率的预测因素。
2000 年 1 月至 2011 年 12 月期间,共纳入 227 例 COPD 患者进行前瞻性临床研究。在入组前一年和此后每年记录报告的加重次数,并根据中位年加重频率将患者分为加重频率低(每年少于一次加重)和高(每年一次或多次加重)两组。在加重频率高的患者中,进一步分为中度频繁加重(每年少于两次加重)和重度频繁加重(每年两次或更多次加重)。记录了 10 年内的临床复发率和生存率。每位患者的平均随访时间为 5.15 年。
在经历低、中、重度频繁加重的患者中,入组前一年的中位数加重次数分别为 0.0、0.5、1.0,更频繁的加重与较低的基线 1 秒用力呼气量(FEV1)(分别为 0.81L、0.75L 和 0.66L)、更高的合并症(分别为 70.7%、75.0%和 89.4%)和住院期间更高的 NPPV 使用率(分别为 16.4%、35.9%和 51.1%)相关。FEV1 下降和死亡率随加重频率的增加而增加。
加重频率可用于生成离散的患者亚群,支持存在多种 COPD 表型的假说,并可用于患者风险分层。