Dai Wangde, Cheung Elissa, Alleman Rick J, Perry Justin B, Allen Mitchell E, Brown David A, Kloner Robert A
HMRI Cardiovascular Research Institute, Huntington Medical Research Institutes, 10 Pico Street, Pasadena, CA, 91105, USA.
Division of Cardiovascular Medicine of the Keck School of Medicine, University of Southern California, Los Angeles, California, 90017-2395, USA.
Cardiovasc Drugs Ther. 2016 Dec;30(6):559-566. doi: 10.1007/s10557-016-6695-9.
Dysfunctional mitochondria are considered to be the major source of intracellular reactive oxygen species and play a central role in the pathophysiology of myocardial ischemia/reperfusion. This study sought to determine effects of mitochondria-targeted cytoprotective peptide SBT-20 on myocardial infarct size in two different models of ischemia/reperfusion.
For in vivo studies, anesthetized Sprague Dawley rats were subjected to 30 min of coronary artery occlusion followed by 3 h of reperfusion. Rats received saline (control), low dose SBT-20 (0.3 mg/kg/h) or high dose SBT-20 (3 mg/kg/h) treatment (n = 15 rats in each group). Saline or SBT-20 were delivered into the jugular vein starting 5 min after coronary artery occlusion and were continued for one hour post coronary artery reperfusion. Body temperature, heart rate and blood pressure were monitored during the procedure. At the end of 3 h reperfusion, the ischemic risk area, no-reflow area, and infarct size were measured. In separate in vitro studies, isolated rat hearts were exposed to 20 min global ischemia, followed by SBT-20 administration (1 μM) or no SBT-20 (control) throughout the 2 h reperfusion. In vitro studies were conducted in cells and heart mitochondria to ascertain the mitochondrial effects of SBT-20 on mitochondrial respiration and reactive oxygen species production.
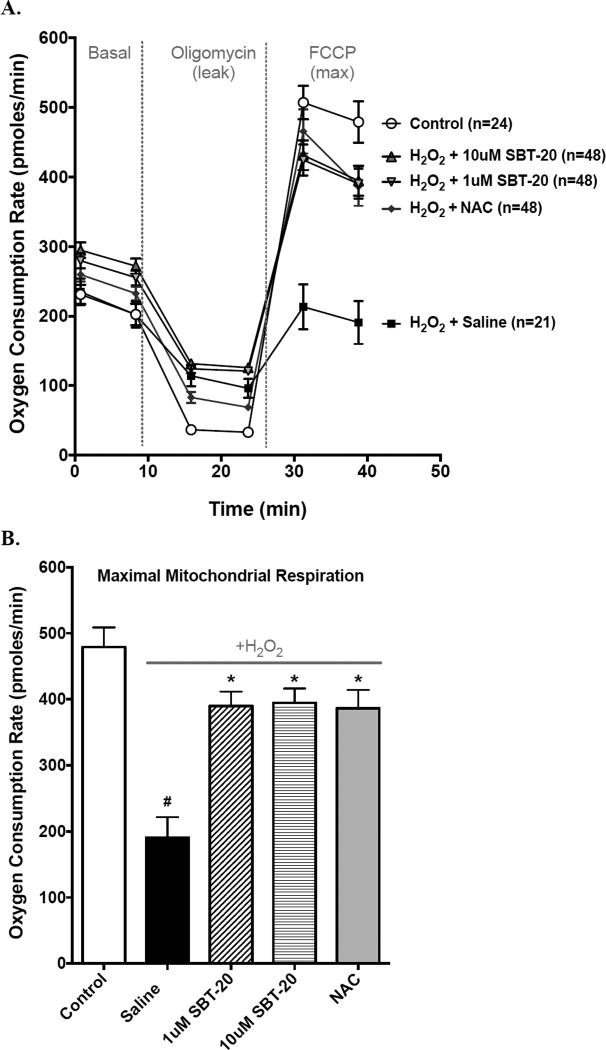
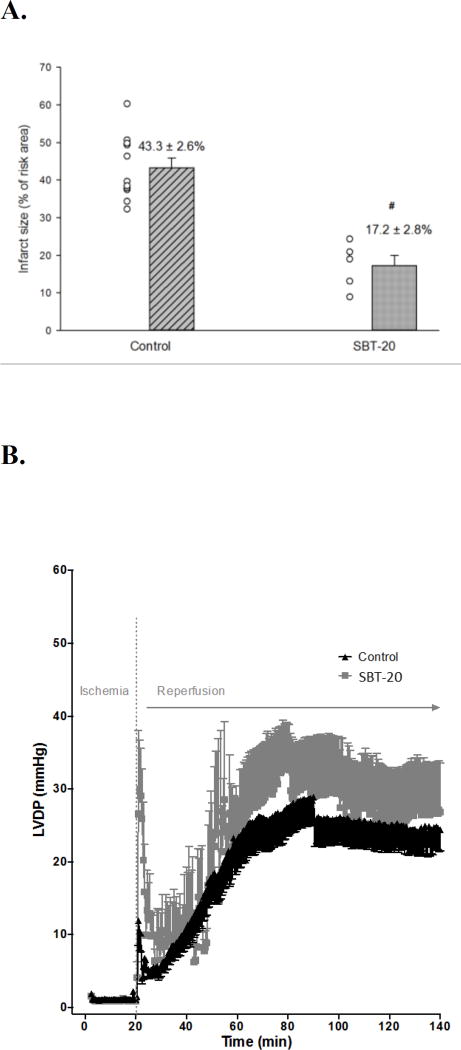
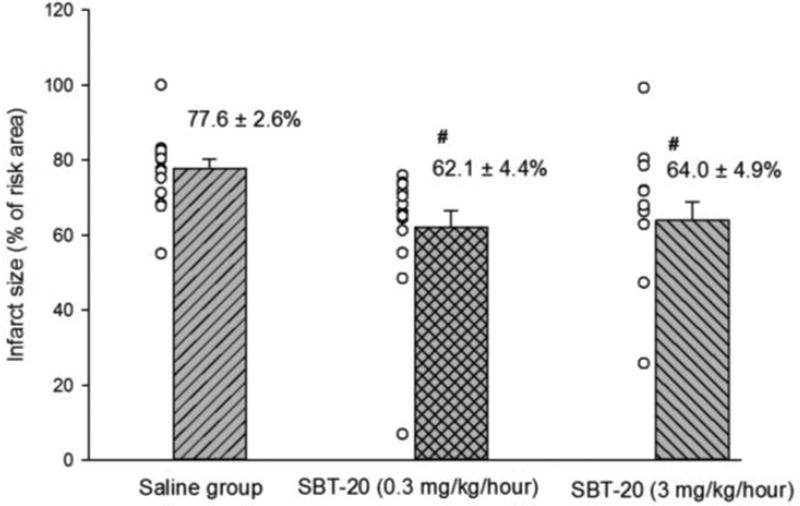
In the in vivo study, the ischemic risk areas (as a percentage of the left ventricle) were similar among the saline (49.5 ± 2.3 %), low dose SBT-20 (48.6 ± 2.1 %), and high dose SBT-20 groups (48.7 ± 3.0 %). Treatment with SBT-20 significantly reduced infarct size ( as a percentage of risk area) in low dose (62.1 ± 4.4 %) and high dose (64.0 ± 4.9 %) compared with saline treatment (77.6 ± 2.6 %, p = 0.001 for both doses). There was no difference in infarct size between low and high dose SBT-20 treatment. The no-reflow areas (as a percentage of the risk area) were comparable among the saline (23.9 ± 1.7 %), low dose SBT-20 (23.7 ± 2.8 %), and high dose groups (25.0 ± 2.1 %). Body temperature, heart rate and blood pressure were comparable among the 3 groups at baseline, during ischemia, and at the end of 3 h of reperfusion. In the in vitro study, infarct size was reduced from 43.3 ± 2.6 % in control group (n = 11) to 17.2 ± 2.8 % in the SBT-20 treatment group (n = 5, p < 0.05). There were no benefits of SBT-20 on recovery of left ventricular developed pressure, coronary flow, or maximal rates of contraction/relaxation. In cell studies, treatment with SBT-20 significantly improved maximal mitochondrial respiration in response to an H2O2 challenge. In isolated mitochondria, reactive oxygen species production was significantly blunted following treatment with SBT-20.
In summary, SBT-20 significantly reduced infarct size in two different models of myocardial injury, but did not affect hemodynamics or no-reflow area in rat heart. The reduction in injury is postulated to involve stabilization of mitochondrial function and reduced mitochondrial production of ROS.
功能失调的线粒体被认为是细胞内活性氧的主要来源,在心肌缺血/再灌注的病理生理学中起核心作用。本研究旨在确定线粒体靶向细胞保护肽SBT-20在两种不同的缺血/再灌注模型中对心肌梗死面积的影响。
在体内研究中,将麻醉的Sprague Dawley大鼠冠状动脉闭塞30分钟,然后再灌注3小时。大鼠接受生理盐水(对照组)、低剂量SBT-20(0.3mg/kg/h)或高剂量SBT-20(3mg/kg/h)治疗(每组15只大鼠)。从冠状动脉闭塞后5分钟开始,将生理盐水或SBT-20经颈静脉给药,并在冠状动脉再灌注后持续1小时。在手术过程中监测体温、心率和血压。在再灌注3小时结束时,测量缺血危险区、无复流区和梗死面积。在单独的体外研究中,将离体大鼠心脏暴露于20分钟全心缺血,然后在整个2小时再灌注过程中给予SBT-20(1μM)或不给予SBT-20(对照组)。在细胞和心脏线粒体中进行体外研究,以确定SBT-20对线粒体呼吸和活性氧产生的线粒体效应。
在体内研究中,生理盐水组(49.5±2.3%)、低剂量SBT-20组(48.6±2.1%)和高剂量SBT-20组(48.7±3.0%)的缺血危险区(占左心室的百分比)相似。与生理盐水治疗组(77.6±2.6%,两种剂量均p = 0.001)相比,SBT-20治疗显著降低了低剂量(62.1±4.4%)和高剂量(64.0±4.9%)的梗死面积(占危险区的百分比)。低剂量和高剂量SBT-20治疗组之间的梗死面积没有差异。生理盐水组(23.9±1.7%)、低剂量SBT-20组(23.7±2.8%)和高剂量组(25.0±2.1%)之间的无复流区(占危险区的百分比)相当。三组在基线、缺血期间和再灌注3小时结束时的体温、心率和血压相当。在体外研究中,梗死面积从对照组(n = 11)的43.3±2.6%降至SBT-20治疗组(n = 5,p < 0.05)的17.2±2.8%。SBT-20对左心室舒张末压、冠状动脉血流或最大收缩/舒张速率的恢复没有益处。在细胞研究中,SBT-20治疗显著改善了对H2O2刺激的最大线粒体呼吸。在分离的线粒体中,SBT-20治疗后活性氧的产生显著减弱。
总之,SBT-20在两种不同的心肌损伤模型中显著减小了梗死面积,但不影响大鼠心脏的血流动力学或无复流区。推测损伤的减轻涉及线粒体功能的稳定和线粒体活性氧产生的减少。