Lu Lin, Ehmke Ross C, Schwartz Lawrence H, Zhao Binsheng
Department of Radiology, Columbia University Medical Center, New York, NY, United States of America.
Department of Medicine, Columbia University Medical Center, New York, NY, United States of America.
PLoS One. 2016 Dec 29;11(12):e0166550. doi: 10.1371/journal.pone.0166550. eCollection 2016.
Radiomics utilizes quantitative image features (QIFs) to characterize tumor phenotype. In practice, radiological images are obtained from different vendors' equipment using various imaging acquisition settings. Our objective was to assess the inter-setting agreement of QIFs computed from CT images by varying two parameters, slice thickness and reconstruction algorithm.
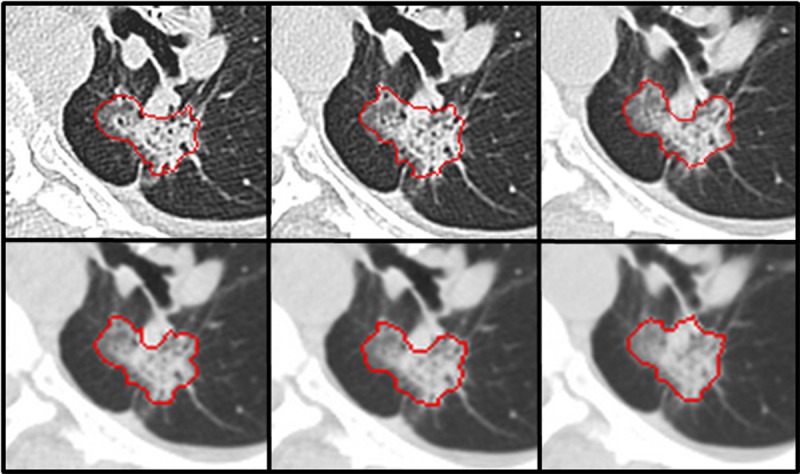
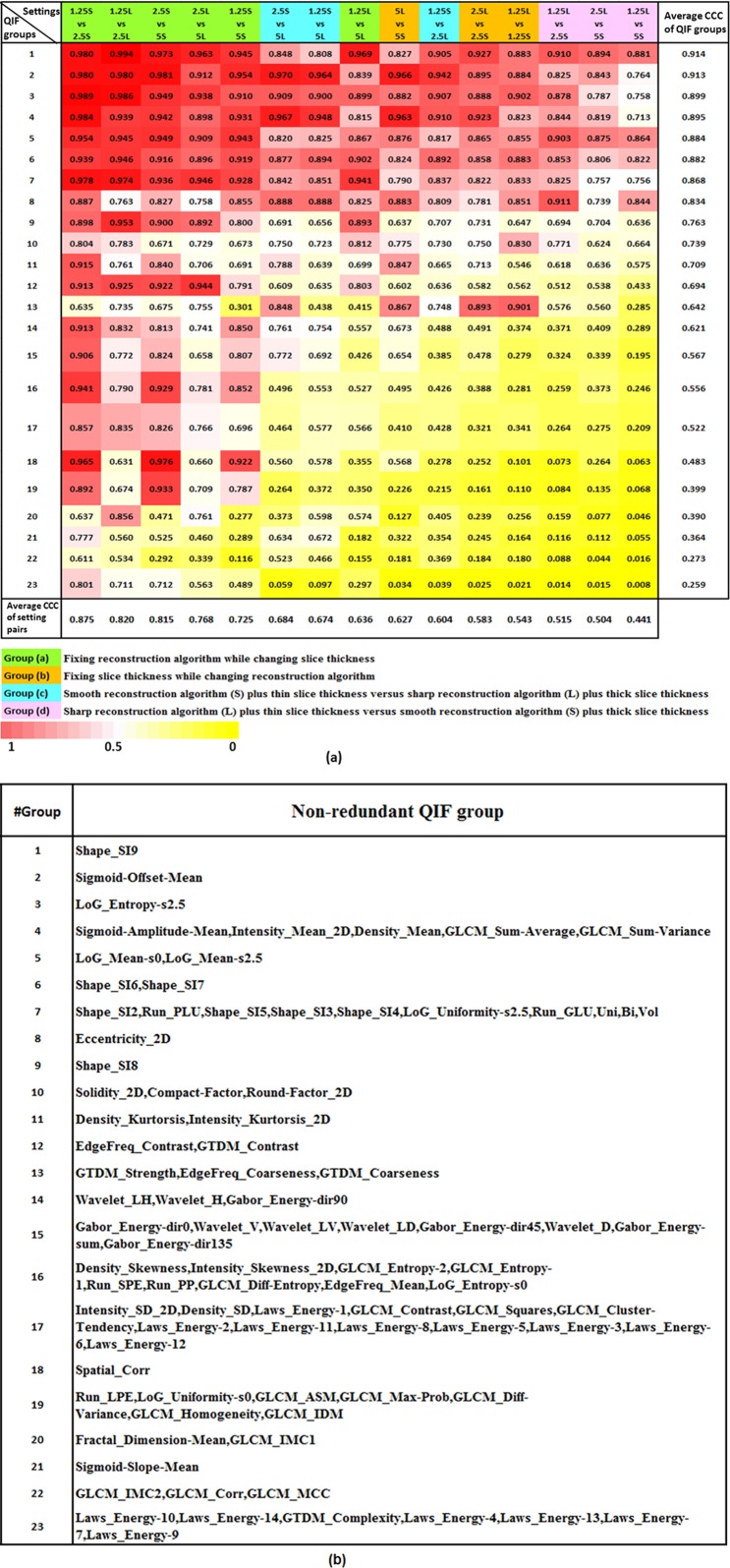
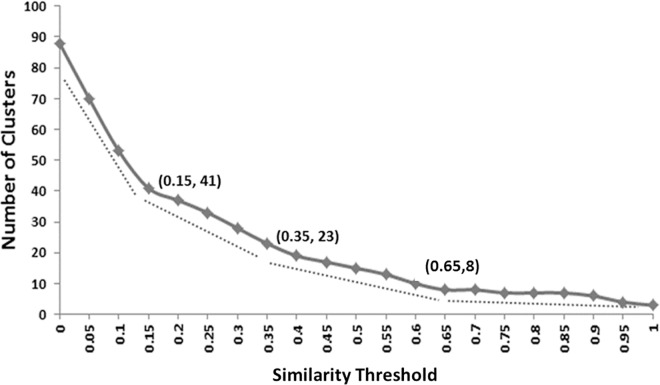
CT images from an IRB-approved/HIPAA-compliant study assessing thirty-two lung cancer patients were included for the analysis. Each scan's raw data were reconstructed into six imaging series using combinations of two reconstruction algorithms (Lung[L] and Standard[S]) and three slice thicknesses (1.25mm, 2.5mm and 5mm), i.e., 1.25L, 1.25S, 2.5L, 2.5S, 5L and 5S. For each imaging-setting, 89 well-defined QIFs were computed for each of the 32 tumors (one tumor per patient). The six settings led to 15 inter-setting comparisons (combinatorial pairs). To reduce QIF redundancy, hierarchical clustering was done. Concordance correlation coefficients (CCCs) were used to assess inter-setting agreement of the non-redundant feature groups. The CCC of each group was assessed by averaging CCCs of QIFs in the group.
Twenty-three non-redundant feature groups were created. Across all feature groups, the best inter-setting agreements (CCCs>0.8) were 1.25S vs 2.5S, 1.25L vs 2.5L, and 2.5S vs 5S; the worst (CCCs<0.51) belonged to 1.25L vs 5S and 2.5L vs 5S. Eight of the feature groups related to size, shape, and coarse texture had an average CCC>0.8 across all imaging settings.
Varying degrees of inter-setting disagreements of QIFs exist when features are computed from CT images reconstructed using different algorithms and slice thicknesses. Our findings highlight the importance of harmonizing imaging acquisition for obtaining consistent QIFs to study tumor imaging phonotype.
放射组学利用定量图像特征(QIFs)来表征肿瘤表型。在实际操作中,放射图像是使用各种成像采集设置从不同供应商的设备获取的。我们的目的是通过改变两个参数,即切片厚度和重建算法,来评估从CT图像计算得到的QIFs的不同设置之间的一致性。
纳入一项经机构审查委员会批准/符合健康保险流通与责任法案的研究中的32例肺癌患者的CT图像进行分析。使用两种重建算法(肺[L]和标准[S])和三种切片厚度(1.25mm、2.5mm和5mm)的组合,将每次扫描的原始数据重建为六个成像系列,即1.25L、1.25S、2.5L、2.5S、5L和5S。对于每个成像设置,为32个肿瘤中的每一个(每位患者一个肿瘤)计算89个定义明确的QIFs。这六个设置导致15种不同设置之间的比较(组合对)。为减少QIF冗余,进行了层次聚类。一致性相关系数(CCC)用于评估非冗余特征组的不同设置之间的一致性。通过对组内QIFs的CCC进行平均来评估每个组的CCC。
创建了23个非冗余特征组。在所有特征组中,不同设置之间最佳的一致性(CCC>0.8)为1.25S与2.5S、1.25L与2.5L以及2.5S与5S;最差的(CCC<0.51)是1.25L与5S以及2.5L与5S。在所有成像设置中,与大小、形状和粗糙纹理相关的八个特征组的平均CCC>0.8。
当从使用不同算法和切片厚度重建的CT图像计算特征时,QIFs在不同设置之间存在不同程度的不一致。我们的研究结果强调了统一成像采集对于获得一致的QIFs以研究肿瘤成像表型的重要性。