MRC Integrative Epidemiology Unit, University of Bristol, Bristol, UK.
School of Social and Community Medicine, University of Bristol, Bristol, UK.
Mol Psychiatry. 2018 Feb;23(2):263-270. doi: 10.1038/mp.2016.198. Epub 2017 Jan 3.
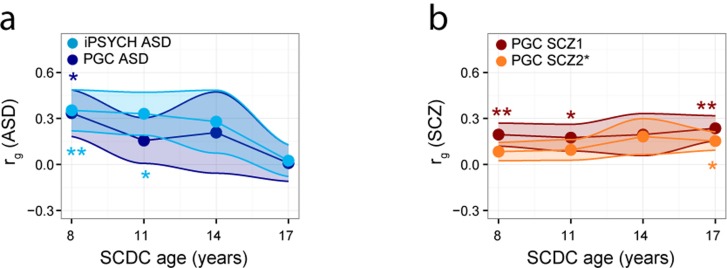
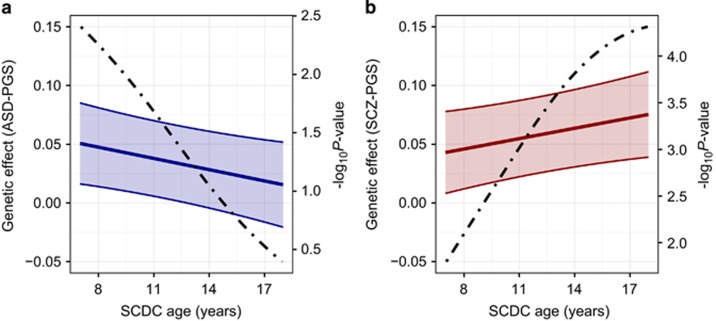
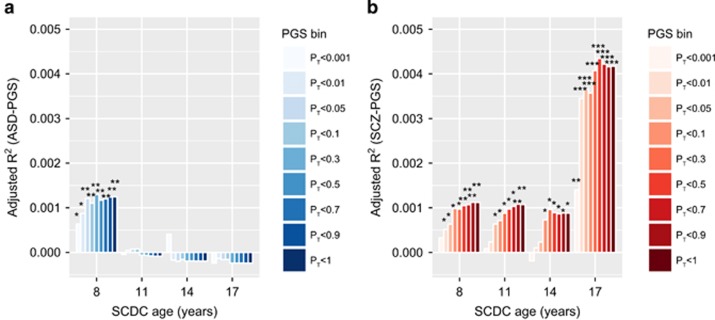
Difficulties in social communication are part of the phenotypic overlap between autism spectrum disorders (ASD) and schizophrenia. Both conditions follow, however, distinct developmental patterns. Symptoms of ASD typically occur during early childhood, whereas most symptoms characteristic of schizophrenia do not appear before early adulthood. We investigated whether overlap in common genetic influences between these clinical conditions and impairments in social communication depends on the developmental stage of the assessed trait. Social communication difficulties were measured in typically-developing youth (Avon Longitudinal Study of Parents and Children, N⩽5553, longitudinal assessments at 8, 11, 14 and 17 years) using the Social Communication Disorder Checklist. Data on clinical ASD (PGC-ASD: 5305 cases, 5305 pseudo-controls; iPSYCH-ASD: 7783 cases, 11 359 controls) and schizophrenia (PGC-SCZ2: 34 241 cases, 45 604 controls, 1235 trios) were either obtained through the Psychiatric Genomics Consortium (PGC) or the Danish iPSYCH project. Overlap in genetic influences between ASD and social communication difficulties during development decreased with age, both in the PGC-ASD and the iPSYCH-ASD sample. Genetic overlap between schizophrenia and social communication difficulties, by contrast, persisted across age, as observed within two independent PGC-SCZ2 subsamples, and showed an increase in magnitude for traits assessed during later adolescence. ASD- and schizophrenia-related polygenic effects were unrelated to each other and changes in trait-disorder links reflect the heterogeneity of genetic factors influencing social communication difficulties during childhood versus later adolescence. Thus, both clinical ASD and schizophrenia share some genetic influences with impairments in social communication, but reveal distinct developmental profiles in their genetic links, consistent with the onset of clinical symptoms.
社交沟通困难是自闭症谱系障碍(ASD)和精神分裂症表型重叠的一部分。然而,这两种情况都遵循不同的发展模式。ASD 的症状通常在儿童早期出现,而大多数精神分裂症的特征症状则不会在成年早期之前出现。我们研究了这些临床病症之间共同遗传影响的重叠以及社交沟通障碍是否取决于所评估特征的发育阶段。使用社交沟通障碍清单(Social Communication Disorder Checklist),在发育正常的青少年中(雅芳纵向父母与子女研究,N⩽5553,在 8、11、14 和 17 岁进行纵向评估)测量社交沟通困难。关于临床 ASD(PGC-ASD:5305 例病例,5305 个假对照;iPSYCH-ASD:7783 例病例,11359 个对照)和精神分裂症(PGC-SCZ2:34241 例病例,45604 个对照,1235 个三胞胎)的数据来自精神疾病基因组学联盟(PGC)或丹麦 iPSYCH 项目。PGC-ASD 和 iPSYCH-ASD 样本中,ASD 与发育过程中社交沟通困难之间的遗传影响重叠随着年龄的增长而降低。相比之下,精神分裂症与社交沟通困难之间的遗传重叠在不同年龄之间持续存在,在两个独立的 PGC-SCZ2 子样本中观察到,并且在评估青春期后期特征时,遗传重叠的幅度增加。ASD 和精神分裂症相关的多基因效应彼此无关,特征-障碍关联的变化反映了影响儿童期和青春期后期社交沟通困难的遗传因素的异质性。因此,临床 ASD 和精神分裂症都与社交沟通障碍存在一些遗传影响,但在遗传关联方面表现出不同的发育模式,与临床症状的出现一致。