Degli Esposti Luca, Favalli Ennio Giulio, Sangiorgi Diego, Di Turi Roberta, Farina Giuseppina, Gambera Marco, Ravasio Roberto
CliCon S.r.l. - Health, Economics & Outcomes Research, Ravenna.
Department of Rheumatology, Istituto Ortopedico Gaetano Pini, Milan.
Clinicoecon Outcomes Res. 2016 Dec 21;9:9-17. doi: 10.2147/CEOR.S108730. eCollection 2017.
The aim of this analysis was to provide an estimate of drug utilization indicators (persistence, switch rate and drug consumption) on biologics and the corresponding costs (drugs, admissions and specialist care) incurred by the Italian National Health Service in the management of adult patients with rheumatoid arthritis (RA).
We conducted an observational retrospective cohort analysis using the administrative databases of three local health units. We considered all patients aged ≥18 years with a diagnosis of RA and at least one biologic drug prescription between January 2010 and December 2012 (recruitment period). Persistence was defined as maintenance over the last 3 months of the follow-up period of the same biological therapy administered at the index date. A switch was defined as the presence of a biological therapy other than that administered at the index date during the last 3 months of the follow-up period. Hospital admissions (with a diagnosis of RA or other RA-related diagnoses), specialist outpatient services, instrumental diagnostics and pharmaceutical consumption were assessed.
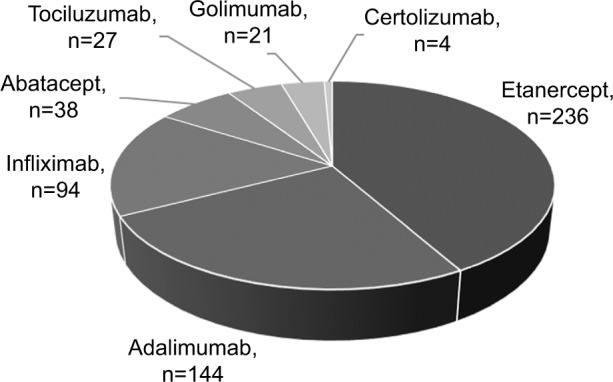
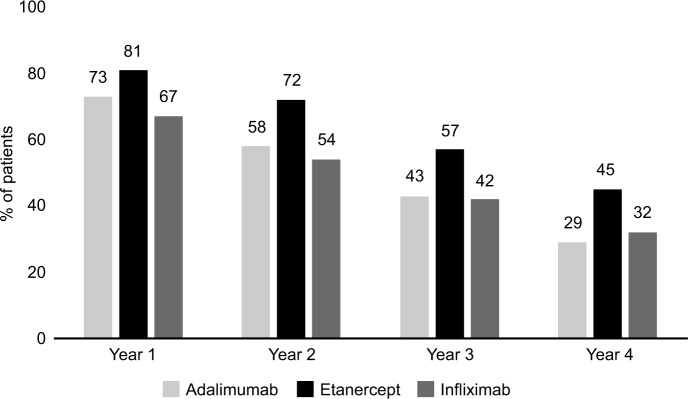
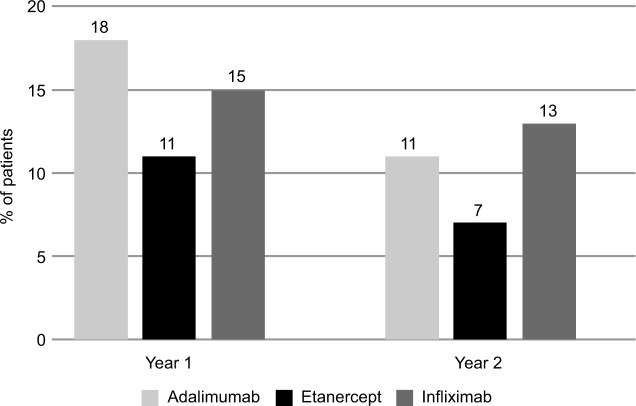
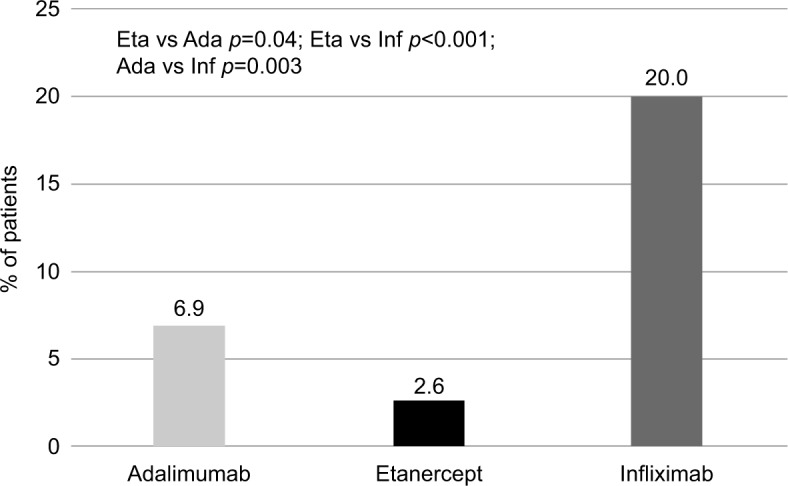
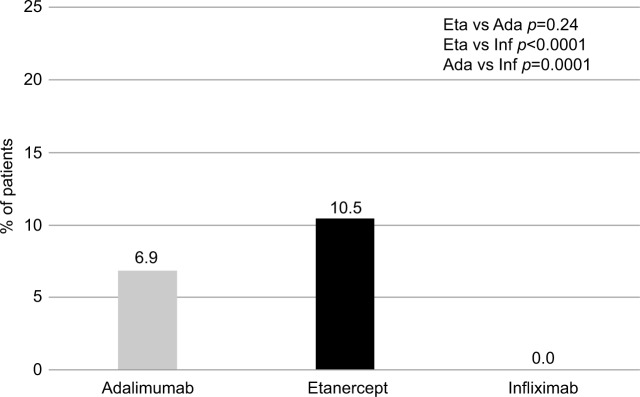
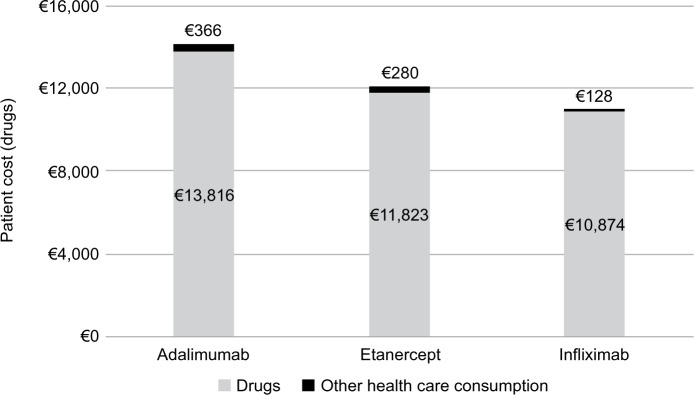
The drug utilization analysis took into account only biologics with at least 90 patients on treatment at baseline (adalimumab n=144, etanercept n=236 and infliximab n=94). In each year, etanercept showed better persistence with initial treatment than adalimumab or infliximab. Etanercept was characterized by the lowest number of patients increasing the initial drug consumption (2.6%) and by the highest number of patients reducing the initial drug consumption (10.5%). The mean cost of treatment for a patient persisting with the initial treatment was €12,388 (€14,182 for adalimumab, €12,103 for etanercept and €11,002 for infliximab). The treatment costs for patients switching from initial treatment during the first year of follow-up were higher than for patients who did not switch (€12,710 vs. €11,332).
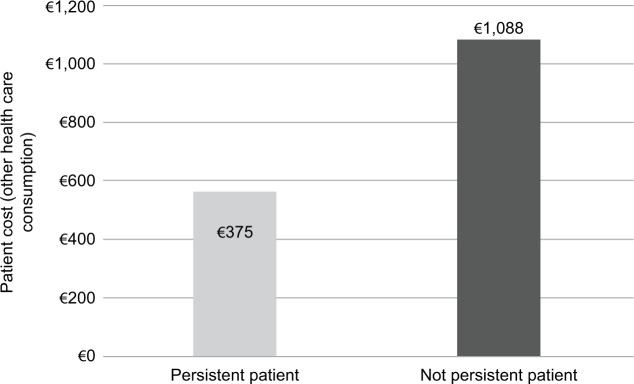
Persistence, switch rate and drug consumption seem to directly influence treatment costs. In subjects not persisting with initial treatment, other health care costs were approximately three times higher than for persistent patients. This difference could suggest a positive effect on the quality of life for persistent patients. Etanercept showed the highest persistence with treatment.
本分析旨在估算意大利国家医疗服务体系在管理成年类风湿关节炎(RA)患者时,生物制剂的药物利用指标(持续用药率、换药率和药物消耗量)以及相应成本(药物、住院和专科护理)。
我们利用三个地方卫生单位的行政数据库进行了一项观察性回顾性队列分析。我们纳入了所有年龄≥18岁、在2010年1月至2012年12月期间(招募期)被诊断为RA且至少有一次生物制剂处方的患者。持续用药定义为在随访期的最后3个月维持在索引日期所使用的相同生物治疗方案。换药定义为在随访期的最后3个月使用了除索引日期所使用的生物治疗方案以外的其他生物治疗方案。评估了住院情况(诊断为RA或其他与RA相关的诊断)、专科门诊服务、仪器诊断和药物消耗情况。
药物利用分析仅考虑了基线时至少有90名患者接受治疗的生物制剂(阿达木单抗n = 144、依那西普n = 236和英夫利昔单抗n = 94)。每年,依那西普在初始治疗中的持续用药率均高于阿达木单抗或英夫利昔单抗。依那西普的特点是增加初始药物消耗量的患者数量最少(2.6%),减少初始药物消耗量的患者数量最多(10.5%)。持续接受初始治疗的患者的平均治疗成本为12,388欧元(阿达木单抗为14,182欧元,依那西普为12,103欧元,英夫利昔单抗为11,002欧元)。随访第一年从初始治疗换药的患者的治疗成本高于未换药的患者(12,710欧元对11,332欧元)。
持续用药率、换药率和药物消耗量似乎直接影响治疗成本。在未持续接受初始治疗的患者中,其他医疗保健成本比持续用药的患者高出约三倍。这种差异可能表明持续用药的患者生活质量有积极影响。依那西普在治疗中显示出最高的持续用药率。