Allardet-Servent Jérôme, Lebsir Melissa, Dubroca Christian, Fabrigoule Martine, Jordana Sylvie, Signouret Thomas, Castanier Matthias, Thomas Guillemette, Soundaravelou Rettinavelou, Lepidi Anne, Delapierre Laurence, Penaranda Guillaume, Halfon Philippe, Seghboyan Jean-Marie
Service de Réanimation, Hôpital Européen Marseille, Marseille, France.
Laboratoire Européen, Laboratoire de Biologie Spécialisée Alphabio, Marseille, France.
PLoS One. 2017 Jan 10;12(1):e0169593. doi: 10.1371/journal.pone.0169593. eCollection 2017.
Rapid detection of abnormal biological values using point-of-care (POC) testing allows clinicians to promptly initiate therapy; however, there are concerns regarding the reliability of POC measurements. We investigated the agreement between the latest generation blood gas analyzer and central laboratory measurements of electrolytes, bicarbonate, hemoglobin, hematocrit, and glucose.
314 paired samples were collected prospectively from 51 critically ill patients. All samples were drawn simultaneously in the morning from an arterial line. BD Vacutainer tubes were analyzed in the central laboratory using Beckman Coulter analyzers (AU 5800 and DxH 800). BD Preset 3 ml heparinized-syringes were analyzed immediately in the ICU using the POC Siemens RAPIDPoint 500 blood gas system. We used CLIA proficiency testing criteria to define acceptable analytical performance and interchangeability.
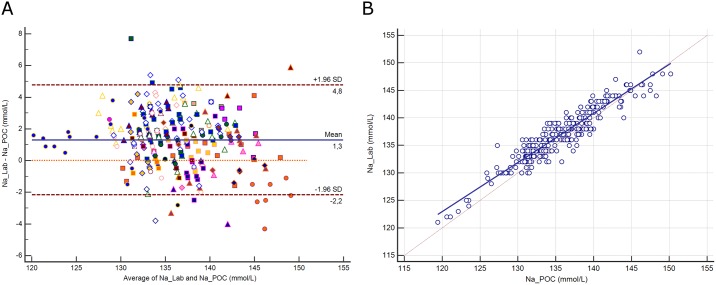
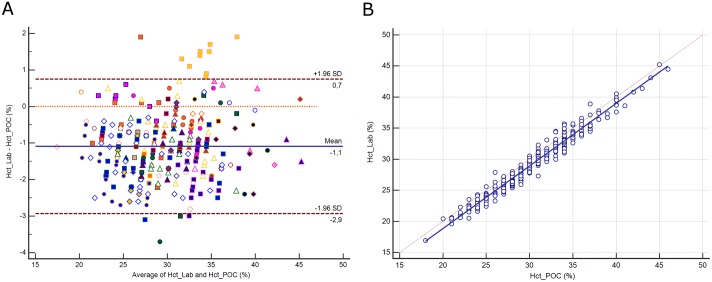
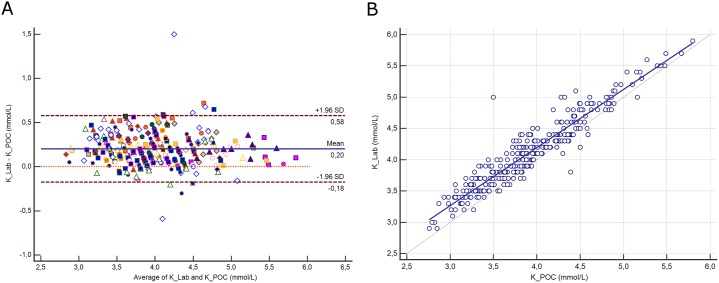
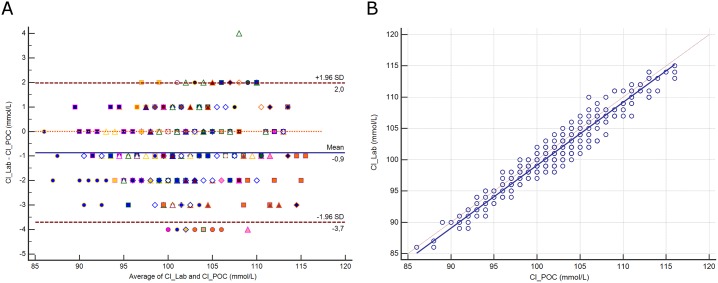
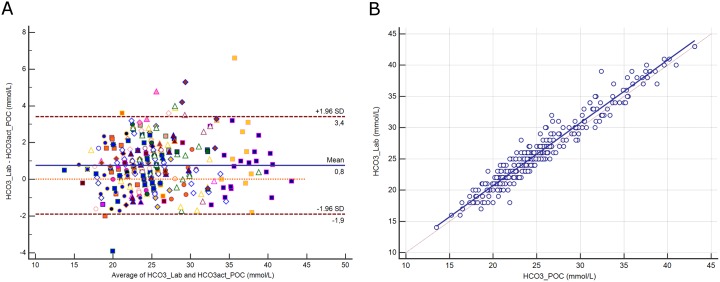
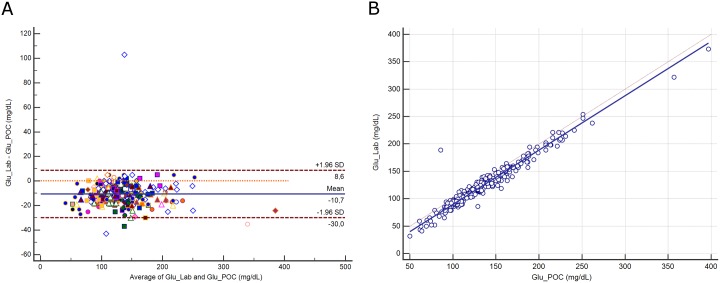
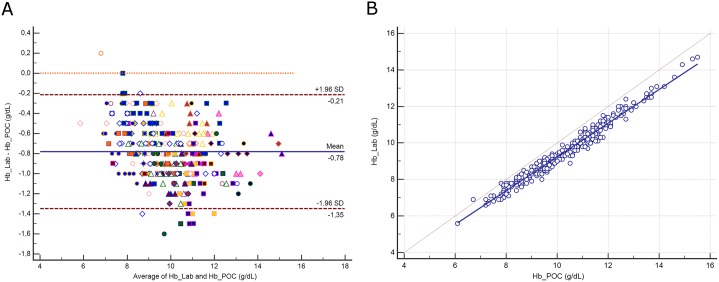
Biases, limits of agreement (±1.96 SD) and coefficients of correlation were respectively: 1.3 (-2.2 to 4.8 mmol/L, r = 0.936) for sodium; 0.2 (-0.2 to 0.6 mmol/L, r = 0.944) for potassium; -0.9 (-3.7 to 2 mmol/L, r = 0.967) for chloride; 0.8 (-1.9 to 3.4 mmol/L, r = 0.968) for bicarbonate; -11 (-30 to 9 mg/dL, r = 0.972) for glucose; -0.8 (-1.4 to -0.2 g/dL, r = 0.985) for hemoglobin; and -1.1 (-2.9 to 0.7%, r = 0.981) for hematocrit. All differences were below CLIA cut-off values, except for hemoglobin.
Compared to central Laboratory analyzers, the POC Siemens RAPIDPoint 500 blood gas system satisfied the CLIA criteria of interchangeability for all tested parameters, except for hemoglobin. These results are warranted for our own procedures and devices. Bearing these restrictions, we recommend clinicians to initiate an appropriate therapy based on POC testing without awaiting a control measurement.
使用即时检验(POC)快速检测异常生物学值可使临床医生迅速开始治疗;然而,人们对POC测量的可靠性存在担忧。我们调查了最新一代血气分析仪与中心实验室对电解质、碳酸氢盐、血红蛋白、血细胞比容和葡萄糖的测量结果之间的一致性。
前瞻性地从51名危重症患者中收集了314对样本。所有样本均于早晨同时从动脉导管采集。BD Vacutainer管在中心实验室使用贝克曼库尔特分析仪(AU 5800和DxH 800)进行分析。BD预设3ml肝素化注射器在重症监护病房(ICU)立即使用POC西门子RAPIDPoint 500血气系统进行分析。我们使用临床实验室改进修正案(CLIA)能力验证标准来定义可接受的分析性能和互换性。
钠的偏差、一致性界限(±1.96标准差)和相关系数分别为:1.3(-2.2至4.8mmol/L,r = 0.936);钾为0.2(-0.2至0.6mmol/L,r = 0.944);氯为-0.9(-3.7至2mmol/L,r = 0.967);碳酸氢盐为0.8(-1.9至3.4mmol/L,r = 0.968);葡萄糖为-11(-30至9mg/dL,r = 0.972);血红蛋白为-0.8(-1.4至-0.2g/dL,r = 0.985);血细胞比容为-1.1(-2.9至0.7%,r = 0.981)。除血红蛋白外,所有差异均低于CLIA临界值。
与中心实验室分析仪相比,POC西门子RAPIDPoint 500血气系统满足CLIA对所有测试参数(血红蛋白除外)的互换性标准。这些结果适用于我们自己的程序和设备。考虑到这些限制,我们建议临床医生根据POC测试开始适当治疗,而无需等待对照测量结果。