Hong Chul Gie, Cho Jae Hwan, Suh Dae Chul, Hwang Chang Ju, Lee Dong-Ho, Lee Choon Sung
Department of Orthopedic Surgery, CHA Gumi Medical Center, Cha University, Gumi, Korea.
Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, 388-1, PungNap-2-dong, SongPa-gu, Seoul, Korea.
World J Surg Oncol. 2017 Feb 14;15(1):45. doi: 10.1186/s12957-017-1118-3.
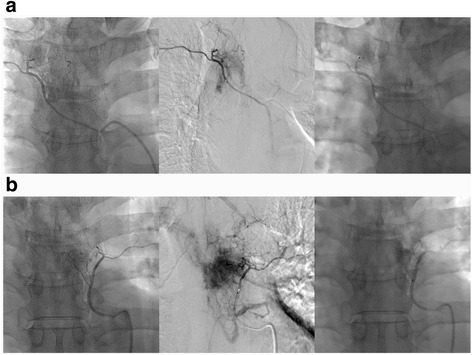
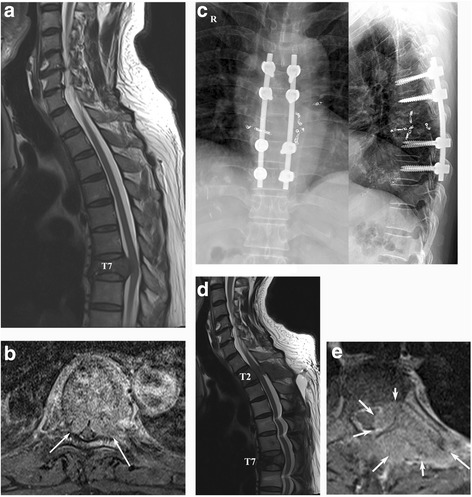
The contribution of preoperative embolization in reducing intraoperative blood loss and its clinical importance are unclear. So, we aimed to compare the perioperative clinical outcomes based on whether preoperative embolization was performed and assess the role and safety of preoperative embolization in metastatic spinal cord compression (MSCC) patients.
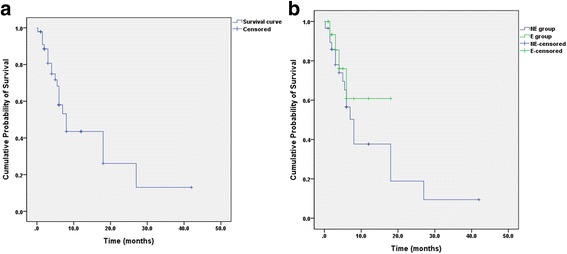
We enrolled 52 patients (men, 37; women, 15) who underwent palliative decompression for MSCC. Demographic data, neurologic status, surgery-related data (operation time, estimated blood loss, and transfusion), complications, and survival time were recorded. Patients were categorized based on whether they received preoperative embolization: groups E (embolization) (n = 18) and NE (non-embolization) (n = 34) and the clinical parameters were compared. Subgroup analysis was performed specifically for cases of hypervascular tumors (23/52, 44%).
The transfusion degree was greater in the NE group (4.6 pints) than in the E group (2.5 pints, P = 0.025); the other parameters did not differ between the groups. However, massive bleeding (>2000 mL) was more frequent in the NE group (10/34) than in the E group (0/18, P = 0.010). Subgroup analysis indicated that intraoperative blood loss was greater in the NE group (1988 mL) than in the E group (1095 mL, P = 0.042) in hypervascular tumor patients. Although massive bleeding was more frequent among hypervascular tumor patients, 3 patients with non-hypervascularized tumors also exhibited massive bleeding (P = 0.087).
Intraoperative blood loss and perioperative transfusion can be reduced by preoperative embolization in MSCC patients. Neurologic recovery, operation time, and complications did not differ according to the application of embolization. As preoperative embolization is relatively safe and effective for controlling intraoperative bleeding without any neurologic deterioration, it is highly recommended for hypervascular tumors. Moreover, it may also be effective for non-hypervascular tumors as massive bleeding may be noted in some cases.
术前栓塞在减少术中失血方面的作用及其临床重要性尚不清楚。因此,我们旨在比较基于是否进行术前栓塞的围手术期临床结局,并评估术前栓塞在转移性脊髓压迫(MSCC)患者中的作用和安全性。
我们纳入了52例行MSCC姑息减压术的患者(男性37例;女性15例)。记录人口统计学数据、神经功能状态、手术相关数据(手术时间、估计失血量和输血情况)、并发症及生存时间。根据患者是否接受术前栓塞进行分组:栓塞组(E组)(n = 18)和非栓塞组(NE组)(n = 34),并比较临床参数。对富血管肿瘤病例(23/52,44%)进行了亚组分析。
NE组的输血量(4.6品脱)多于E组(2.5品脱,P = 0.025);两组的其他参数无差异。然而,NE组(10/34)发生大量出血(>2000 mL)的频率高于E组(0/18,P = 0.010)。亚组分析表明,富血管肿瘤患者中,NE组的术中失血量(1988 mL)多于E组(1095 mL,P = 0.042)。虽然富血管肿瘤患者中大量出血更为常见,但3例非富血管化肿瘤患者也出现了大量出血(P = 0.087)。
术前栓塞可减少MSCC患者的术中失血和围手术期输血。神经功能恢复、手术时间和并发症在是否应用栓塞方面无差异。由于术前栓塞在控制术中出血方面相对安全有效且无任何神经功能恶化,因此强烈推荐用于富血管肿瘤。此外,对于非富血管肿瘤可能也有效,因为在某些情况下可能会出现大量出血。