Fitzpatrick Jane, Bulsara Max K, McCrory Paul Robert, Richardson Martin D, Zheng Ming Hao
School of Surgery, The University of Western Australia, Crawley, Western Australia, Australia.; QEII Medical Centre, Nedlands, Western Australia, Australia.
Chair in Biostatistics, Institute for Health Research, University of Notre Dame, Fremantle, Western Australia, Australia.
Orthop J Sports Med. 2017 Jan 3;5(1):2325967116675272. doi: 10.1177/2325967116675272. eCollection 2017 Jan.
Platelet-rich plasma (PRP) has been extensively used as a treatment in tissue healing in tendinopathy, muscle injury, and osteoarthritis. However, there is variation in methods of extraction, and this produces different types of PRP.
To determine the composition of PRP obtained from 4 commercial separation kits, which would allow assessment of current classification systems used in cross-study comparisons.
Controlled laboratory study.
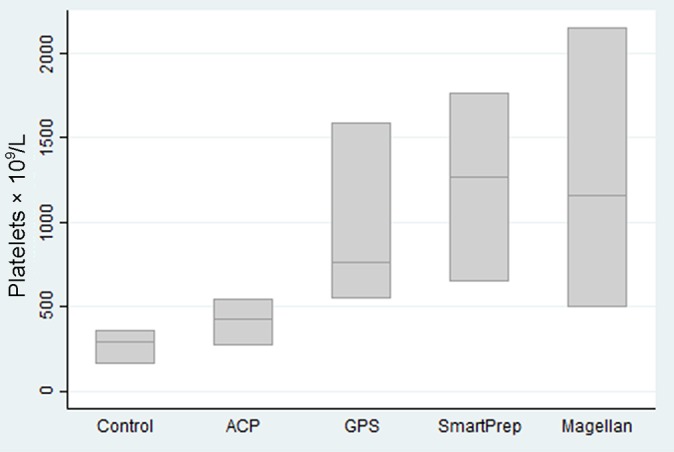
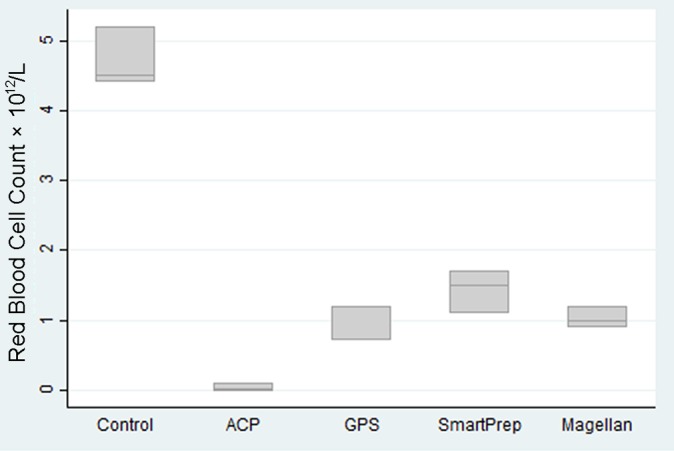
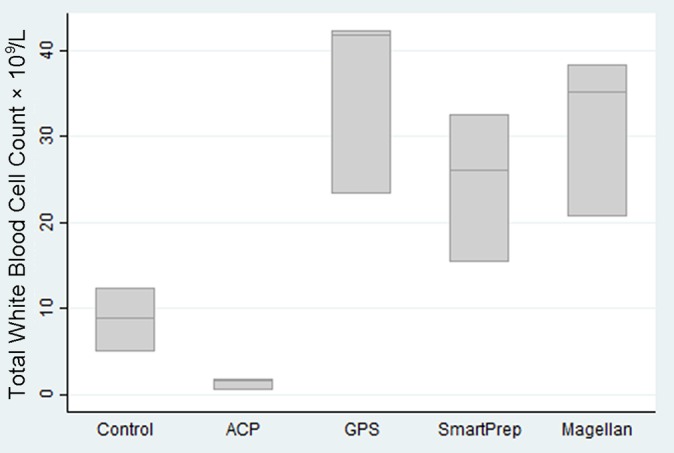
Three normal adults each donated 181 mL of whole blood, some of which served as a control and the remainder of which was processed through 4 PRP separation kits: GPS III (Biomet Biologics), Smart-Prep2 (Harvest Terumo), Magellan (Arteriocyte Medical Systems), and ACP (Device Technologies). The resultant PRP was tested for platelet count, red blood cell count, and white blood cell count, including differential in a commercial pathology laboratory. Glucose and pH measurements were obtained from a blood gas autoanalyzer machine.
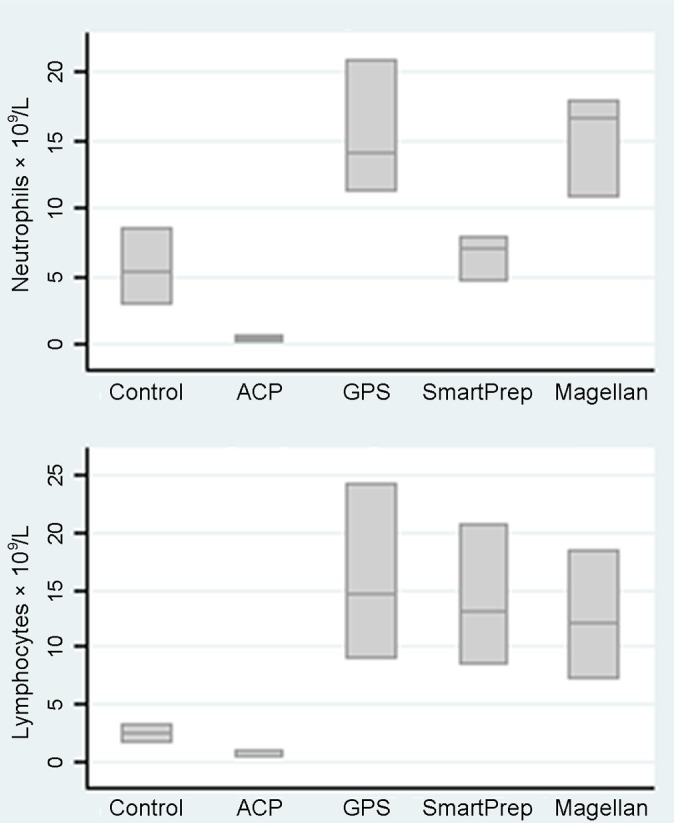
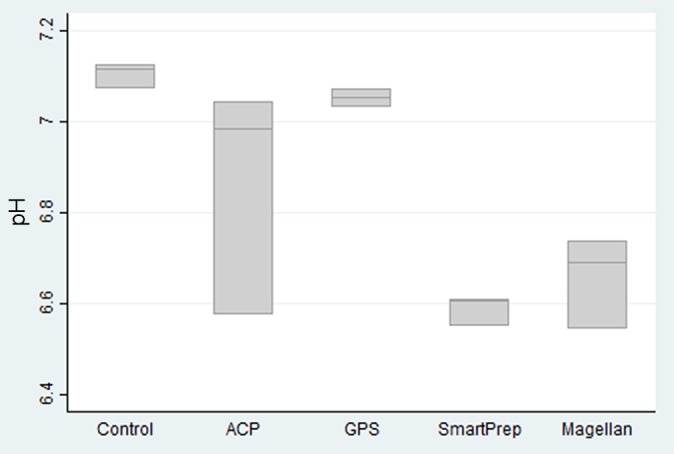
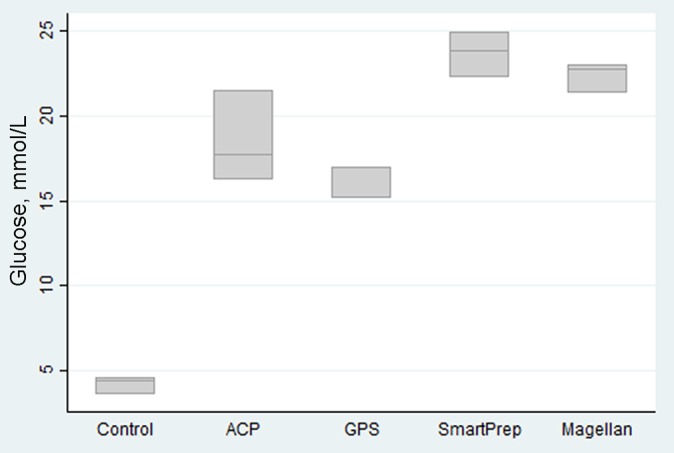
Three kits taking samples from the "buffy coat layer" were found to have greater concentrations of platelets (3-6 times baseline), while 1 kit taking samples from plasma was found to have platelet concentrations of only 1.5 times baseline. The same 3 kits produced an increased concentration of white blood cells (3-6 times baseline); these consisted of neutrophils, leukocytes, and monocytes. This represents high concentrations of platelets and white blood cells. A small drop in pH was thought to relate to the citrate used in the sample preparation. Interestingly, an unexpected increase in glucose concentrations, with 3 to 6 times greater than baseline levels, was found in all samples.
This study reveals the variation of blood components, including platelets, red blood cells, leukocytes, pH, and glucose in PRP extractions. The high concentrations of cells are important, as the white blood cell count in PRP samples has frequently been ignored, being considered insignificant. The lack of standardization of PRP preparation for clinical use has contributed at least in part to the varying clinical efficacy in PRP use.
The variation of platelet and other blood component concentrations between commercial PRP kits may affect clinical treatment outcomes. There is a need for standardization of PRP for clinical use.
富血小板血浆(PRP)已被广泛用于治疗肌腱病、肌肉损伤和骨关节炎中的组织愈合。然而,提取方法存在差异,这导致产生不同类型的PRP。
确定从4种商业分离试剂盒中获得的PRP的成分,这将有助于评估交叉研究比较中使用的当前分类系统。
对照实验室研究。
三名正常成年人每人捐献181毫升全血,其中一些用作对照,其余的通过4种PRP分离试剂盒进行处理:GPS III(Biomet Biologics)、Smart-Prep2(Harvest Terumo)、麦哲伦(Arteriocyte Medical Systems)和ACP(Device Technologies)。所得PRP在商业病理实验室进行血小板计数、红细胞计数和白细胞计数检测,包括分类计数。葡萄糖和pH值测量通过血气自动分析仪获得。
发现从“血沉棕黄层”取样的3种试剂盒的血小板浓度更高(为基线的3至6倍)而从血浆取样的1种试剂盒的血小板浓度仅为基线的1.5倍。同样的3种试剂盒产生的白细胞浓度增加(为基线的3至6倍);这些白细胞包括中性粒细胞、白细胞和单核细胞。这代表了高浓度的血小板和白细胞。pH值略有下降被认为与样品制备中使用的柠檬酸盐有关。有趣的是,在所有样品中均发现葡萄糖浓度意外升高,比基线水平高3至6倍。
本研究揭示了PRP提取中血液成分(包括血小板、红细胞、白细胞、pH值和葡萄糖)的差异。细胞的高浓度很重要,因为PRP样本中的白细胞计数经常被忽视,被认为无关紧要。临床使用的PRP制备缺乏标准化至少部分导致了PRP使用中临床疗效的差异。
商业PRP试剂盒之间血小板和其他血液成分浓度的差异可能会影响临床治疗结果。临床使用的PRP需要标准化。