Minchella Peter A, Chipungu Geoffrey, Kim Andrea A, Sarr Abdoulaye, Ali Hammad, Mwenda Reuben, Nkengasong John N, Singer Daniel
Laboratory Leadership Service assigned to Division of Global HIV and Tuberculosis, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
Division of Global HIV and Tuberculosis, Centers for Disease Control and Prevention, Lilongwe, Malawi.
PLoS One. 2017 Feb 24;12(2):e0173009. doi: 10.1371/journal.pone.0173009. eCollection 2017.
Efforts to reach UNAIDS' treatment and viral suppression targets have increased demand for viral load (VL) testing and strained existing laboratory networks, affecting turnaround time. Longer VL turnaround times delay both initiation of formal adherence counseling and switches to second-line therapy for persons failing treatment and contribute to poorer health outcomes.
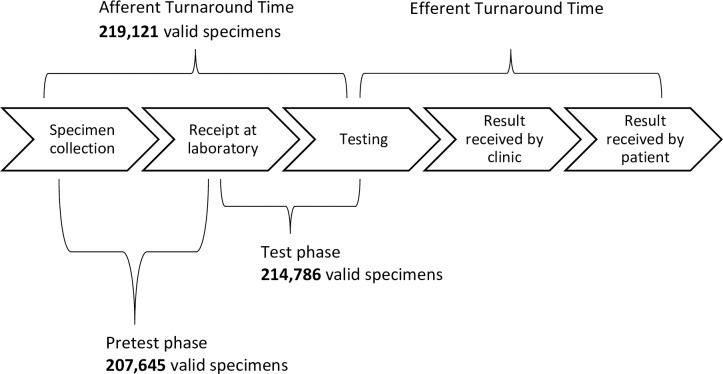
We utilized descriptive statistics and logistic regression to analyze VL testing data collected in Malawi between January 2013 and March 2016. The primary outcomes assessed were greater-than-median pretest phase turnaround time (days elapsed from specimen collection to receipt at the laboratory) and greater-than-median test phase turnaround time (days from receipt to testing).
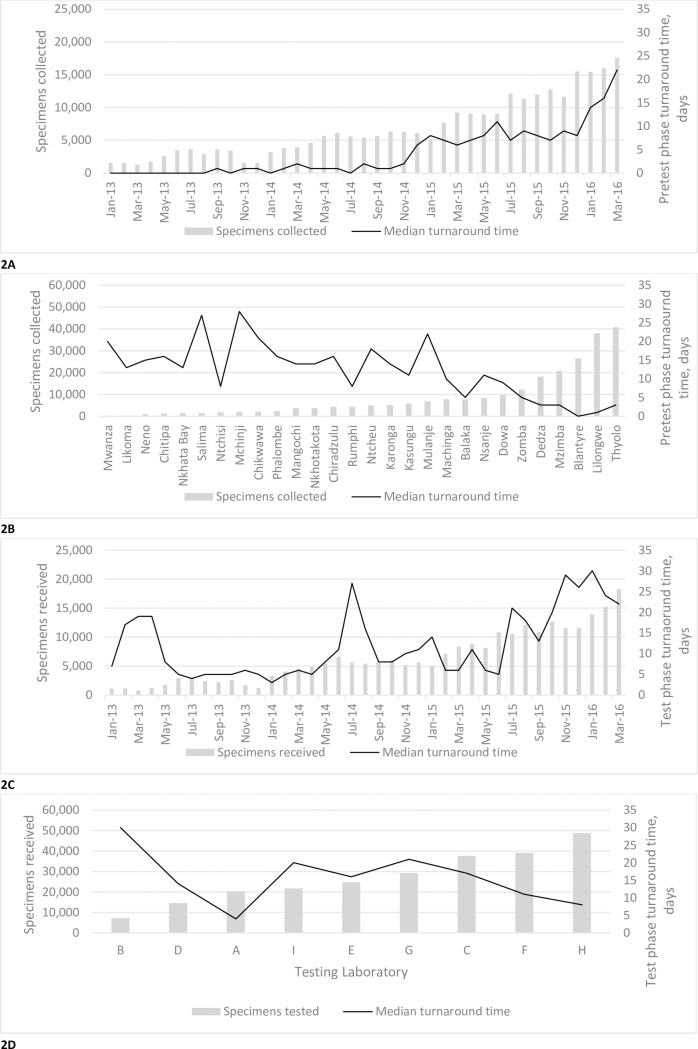
The median number of days between specimen collection and testing increased 3-fold between 2013 (8 days, interquartile range (IQR) = 6-16) and 2015 (24, IQR = 13-39) (p<0.001). Multivariable analysis indicated that the odds of longer pretest phase turnaround time were significantly higher for specimen collection districts without laboratories capable of conducting viral load tests (adjusted odds ratio (aOR) = 5.16; 95% confidence interval (CI) = 5.04-5.27) as well as for Malawi's Northern and Southern regions. Longer test phase turnaround time was significantly associated with use of dried blood spots instead of plasma (aOR = 2.30; 95% CI = 2.23-2.37) and for certain testing months and testing laboratories.
Increased turnaround time for VL testing appeared to be driven in part by categorical factors specific to the phase of turnaround time assessed. Given the implications of longer turnaround time and the global effort to scale up VL testing, addressing these factors via increasing efficiencies, improving quality management systems and generally strengthening the VL spectrum should be considered essential components of controlling the HIV epidemic.
为实现联合国艾滋病规划署的治疗和病毒抑制目标所做的努力增加了对病毒载量(VL)检测的需求,使现有的实验室网络不堪重负,影响了周转时间。较长的VL周转时间既延迟了正式依从性咨询的启动,也延迟了对治疗失败患者转向二线治疗的时间,并导致较差的健康结果。
我们利用描述性统计和逻辑回归分析了2013年1月至2016年3月在马拉维收集的VL检测数据。评估的主要结果是高于中位数的检测前阶段周转时间(从样本采集到实验室收到样本所经过的天数)和高于中位数的检测阶段周转时间(从收到样本到检测的天数)。
2013年(8天,四分位间距(IQR)=6-16)至2015年(24天,IQR=13-39)期间,样本采集与检测之间的中位数天数增加了3倍(p<0.001)。多变量分析表明,对于没有能够进行病毒载量检测的实验室的样本采集地区(调整后的优势比(aOR)=5.16;95%置信区间(CI)=5.04-5.27)以及马拉维的北部和南部地区,检测前阶段周转时间较长的几率显著更高。检测阶段周转时间较长与使用干血斑而非血浆(aOR=2.30;95%CI=2.23-2.37)以及某些检测月份和检测实验室显著相关。
VL检测周转时间的增加似乎部分是由所评估的周转时间阶段特有的分类因素驱动的。鉴于较长周转时间的影响以及全球扩大VL检测的努力,通过提高效率、改进质量管理系统以及总体上加强VL检测范围来解决这些因素应被视为控制艾滋病毒流行的重要组成部分。