Fawibe Ademola Emmanuel, Odeigah Louis O, Saka Mohammed J
Department of Medicine, University of Ilorin/University of Ilorin Teaching Hospital, Ilorin, Nigeria.
Department of Medicine, Faculty of Clinical Sciences, College of health Sciences, University of Ilorin, Ilorin, Kwara State, Nigeria.
BMC Pulm Med. 2017 Mar 6;17(1):48. doi: 10.1186/s12890-017-0390-x.
The increasing importance of pulmonary function testing in diagnosing and managing lung diseases and assessing improvement has necessitated the need for locally derived reference equations from a sample of the general Nigerian population.
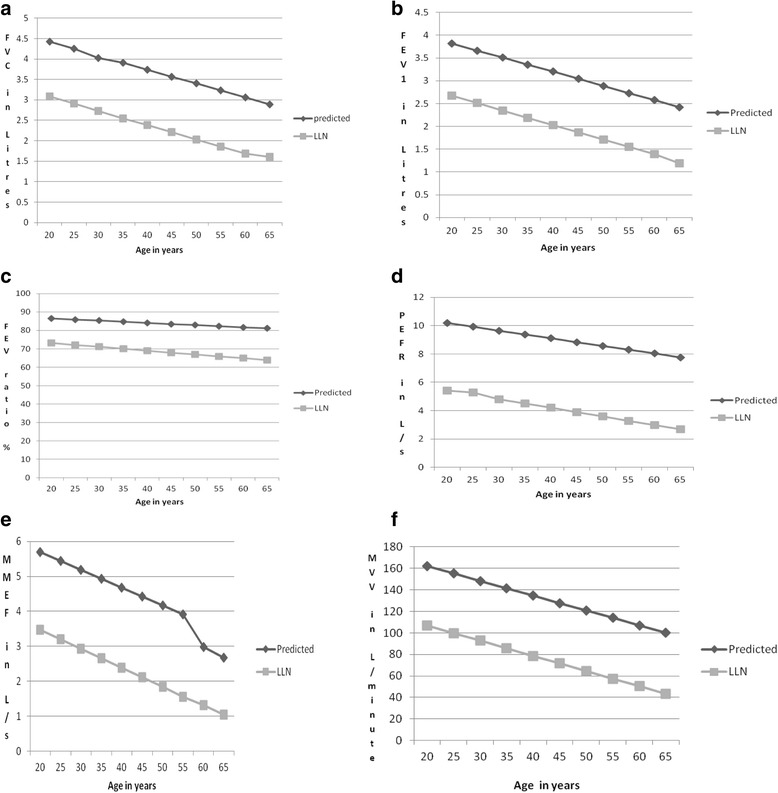
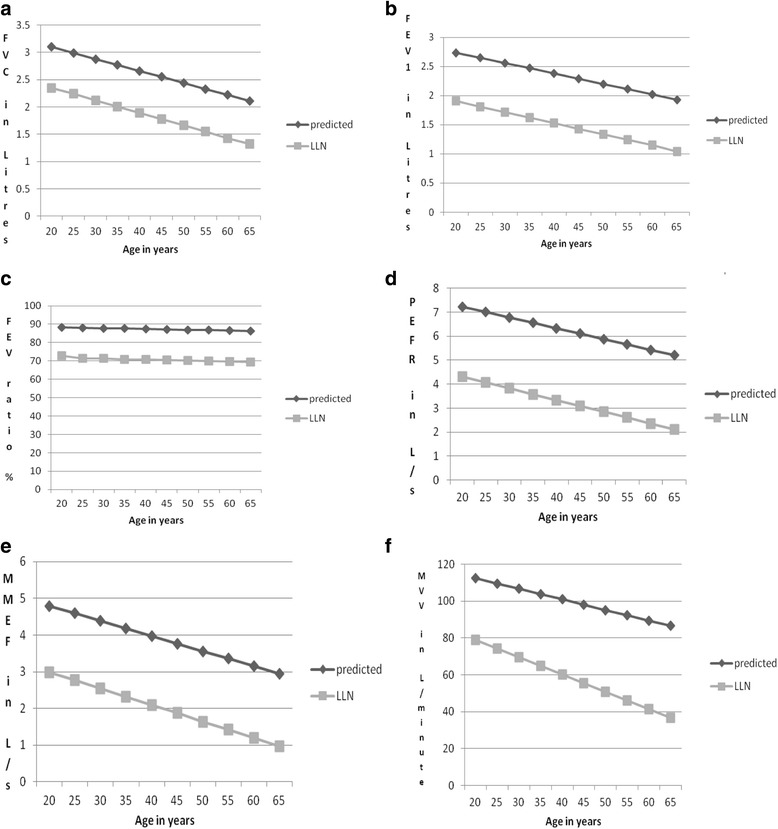
It was a cross sectional study in which we used linear regression models to obtain equations for reference values and lower limits of normal for spirometric indices in adult Nigerians from a sample of the general population aged 18-65 years (males) and 18-63 years (females).
Seven hundred and twenty participants made up of 358 males and 362 females who satisfactorily completed the spirometric measurements using the ATS/ERS reproducibility and acceptability criteria were included in the analysis. The most important predictive variables were height and age. The values of the spirometic indices increase with increasing stature but decrease with increasing age in both sexes. The sex difference in all the indices is also apparent as all the indices, except FEV/FVC, are higher in men than in women. Our values are higher than values obtained from previous studies in Nigeria (except FEV/FVC) but the differences were not statistically significant. This suggests that although the values are increasing, the increase is yet to be significantly different from values obtained using the past equations. The implication of this is that there is need for periodic study to derive new equations so as to recognise when there is significant difference. There was no significant difference between values from our equations and those obtained from study among Ethiopians. Compared to report from Iran, our FVC and FEVvalues (in males and females) as well as PEFR (in females) are significantly lower. Our values are also lower than values from Poland. We also observed disparities between our values and those of Afro Americans from the GLI study.
Our findings show that it is important to always interpret ventilatory function tests in any individual by comparing it with reference values obtained from a well-defined population of healthy subjects of the same ethnic origin in similar geographic location.
肺功能测试在诊断和管理肺部疾病以及评估病情改善方面的重要性日益增加,因此有必要从尼日利亚普通人群样本中得出本地参考方程。
这是一项横断面研究,我们使用线性回归模型,从18 - 65岁(男性)和18 - 63岁(女性)的普通人群样本中得出尼日利亚成年人肺量计指标的参考值方程和正常下限方程。
分析纳入了720名参与者,其中358名男性和362名女性,他们使用美国胸科学会/欧洲呼吸学会的可重复性和可接受性标准,令人满意地完成了肺量计测量。最重要的预测变量是身高和年龄。在两性中,肺量计指标的值随着身高的增加而增加,但随着年龄的增加而降低。除了FEV/FVC外,所有指标在男性中均高于女性,性别差异也很明显。我们的值高于尼日利亚先前研究获得的值(FEV/FVC除外),但差异无统计学意义。这表明,尽管这些值在增加,但与使用过去方程获得的值相比,增加幅度尚未有显著差异。这意味着需要定期进行研究以得出新的方程,以便识别何时存在显著差异。我们方程得出的值与埃塞俄比亚人研究获得的值之间没有显著差异。与伊朗的报告相比,我们的FVC和FEV值(男性和女性)以及PEFR(女性)显著更低。我们的值也低于波兰的值。我们还观察到我们的值与GLI研究中非洲裔美国人的值之间存在差异。
我们的研究结果表明,在对任何个体进行通气功能测试时,将其与从地理位置相似、种族相同的健康受试者明确群体中获得的参考值进行比较来解释测试结果非常重要。