Browne Jorge, Edwards Duncan A, Rhodes Kirsty M, Brimicombe D James, Payne Rupert A
Department of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile.
Primary Care Unit, University of Cambridge, Cambridge, UK.
BMJ Open. 2017 Mar 9;7(3):e012546. doi: 10.1136/bmjopen-2016-012546.
The majority of people with dementia have other long-term diseases, the presence of which may affect the progression and management of dementia. This study aimed to identify subgroups with higher healthcare needs, by analysing how primary care consultations, number of prescriptions and hospital admissions by people with dementia varies with having additional long-term diseases (comorbidity).
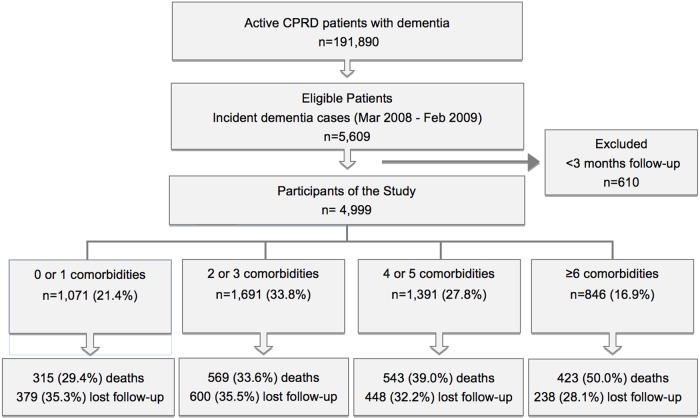
A retrospective cohort study based on health data from the Clinical Practice Research Datalink (CPRD) was conducted. Incident cases of dementia diagnosed in the year starting 1/3/2008 were selected and followed for up to 5 years. The number of comorbidities was obtained from a set of 34 chronic health conditions. Service usage (primary care consultations, hospitalisations and prescriptions) and time-to-death were determined during follow-up. Multilevel negative binomial regression and Cox regression, adjusted for age and gender, were used to model differences in service usage and death between differing numbers of comorbidities.
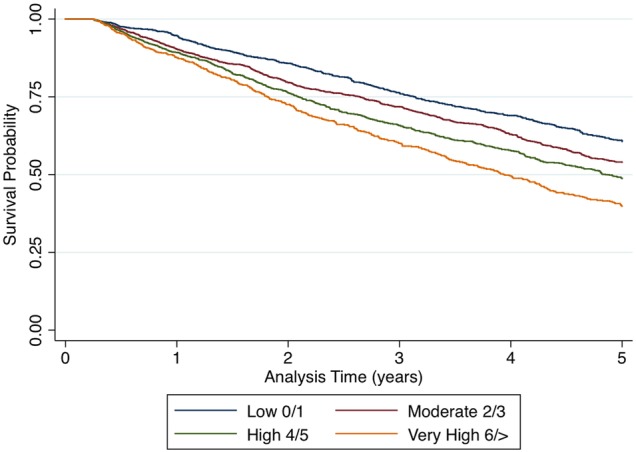
Data from 4999 people (14 866 person-years of follow-up) were analysed. Overall, 91.7% of people had 1 or more additional comorbidities. Compared with those with 2 or 3 comorbidities, people with ≥6 comorbidities had higher rates of primary care consultations (rate ratio (RR) 1.31, 95% CI 1.25 to 1.36), prescriptions (RR 1.68, 95% CI 1.57 to 1.81), and hospitalisation (RR 1.62, 95% CI 1.44 to 1.83), and higher risk of death (HR 1.56, 95% CI 1.37 to 1.78).
In the UK, people with dementia with higher numbers of comorbidities die earlier and have considerably higher health service usage in terms of primary care consultations, hospital admissions and prescribing. This study provides strong evidence that comorbidity is a key factor that should be considered when allocating resources and planning care for people with dementia.
大多数痴呆症患者还患有其他长期疾病,这些疾病的存在可能会影响痴呆症的进展和管理。本研究旨在通过分析痴呆症患者的初级保健会诊、处方数量和住院情况如何随其他长期疾病(合并症)的存在而变化,来确定医疗保健需求较高的亚组。
基于临床实践研究数据链(CPRD)的健康数据进行了一项回顾性队列研究。选取2008年3月1日开始的一年内诊断出的新发痴呆症病例,并随访长达5年。合并症数量来自一组34种慢性健康状况。在随访期间确定服务使用情况(初级保健会诊、住院和处方)以及死亡时间。使用经年龄和性别调整的多水平负二项回归和Cox回归来模拟不同合并症数量之间服务使用和死亡的差异。
分析了4999人的数据(14866人年的随访)。总体而言,91.7%的人有1种或更多其他合并症。与有2种或3种合并症的人相比,有≥6种合并症的人初级保健会诊率更高(率比(RR)1.31,95%置信区间1.25至1.36)、处方率更高(RR 1.68,95%置信区间1.57至1.81)、住院率更高(RR 1.62,95%置信区间1.44至1.83),死亡风险也更高(风险比(HR)1.56,95%置信区间1.37至1.78)。
在英国,合并症数量较多的痴呆症患者死亡更早,在初级保健会诊、住院和开药方面的医疗服务使用率也显著更高。本研究提供了强有力的证据,表明合并症是为痴呆症患者分配资源和规划护理时应考虑的关键因素。