Wu Yuan, Yao Xun, Vespasiani Giacomo, Nicolucci Antonio, Dong Yajie, Kwong Joey, Li Ling, Sun Xin, Tian Haoming, Li Sheyu
Department of Endocrinology and Metabolism, West China Hospital, Sichuan University, Chengdu, China.
Department of Academic Affairs, West China School of Medicine, Sichuan University, Chengdu, China.
JMIR Mhealth Uhealth. 2017 Mar 14;5(3):e35. doi: 10.2196/mhealth.6522.
Mobile health apps for diabetes self-management have different functions. However, the efficacy and safety of each function are not well studied, and no classification is available for these functions.
The aims of this study were to (1) develop and validate a taxonomy of apps for diabetes self-management, (2) investigate the glycemic efficacy of mobile app-based interventions among adults with diabetes in a systematic review of randomized controlled trials (RCTs), and (3) explore the contribution of different function to the effectiveness of entire app-based interventions using the taxonomy.
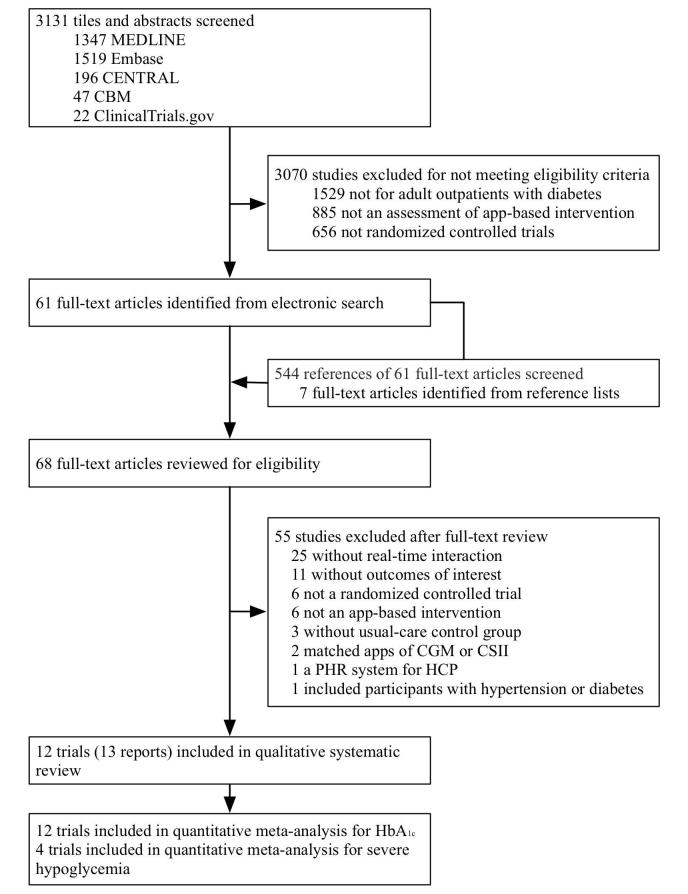
We developed a 3-axis taxonomy with columns of clinical modules, rows of functional modules and cells of functions with risk assessments. This taxonomy was validated by reviewing and classifying commercially available diabetes apps. We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, the Chinese Biomedical Literature Database, and ClinicalTrials.gov from January 2007 to May 2016. We included RCTs of adult outpatients with diabetes that compared using mobile app-based interventions with usual care alone. The mean differences (MDs) in hemoglobin A (HbA) concentrations and risk ratios of adverse events were pooled using a random-effects meta-analysis. After taxonomic classification, we performed exploratory subgroup analyses of the presence or absence of each module across the included app-based interventions.
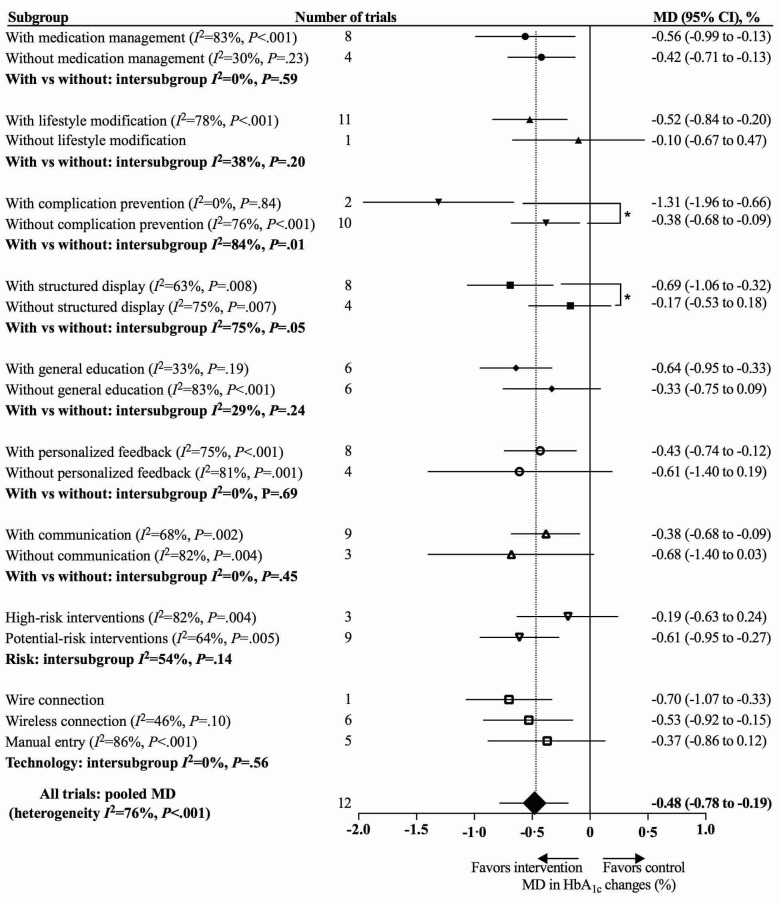
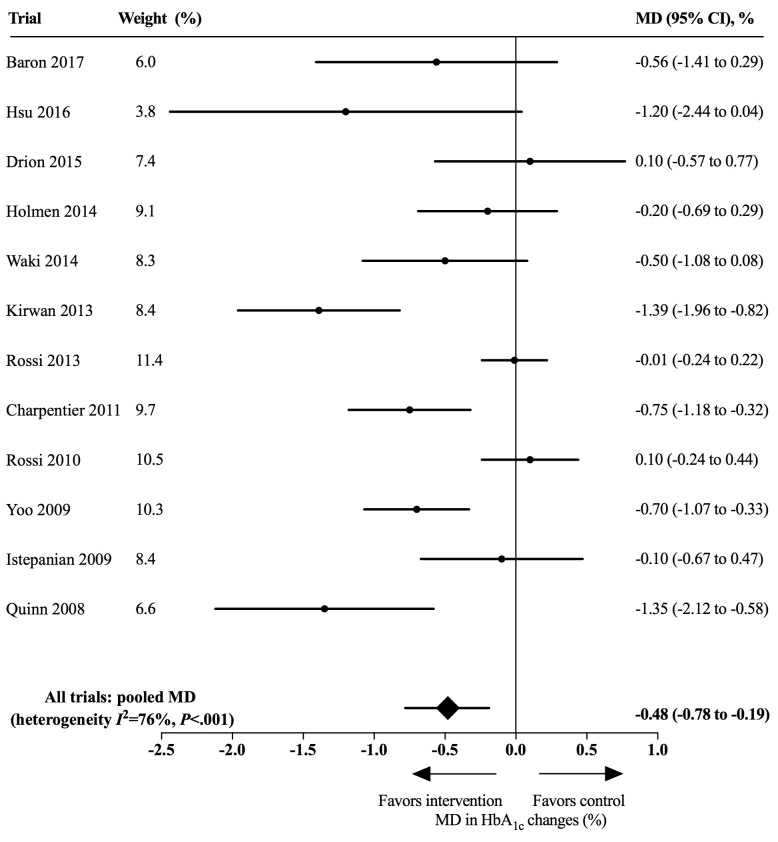
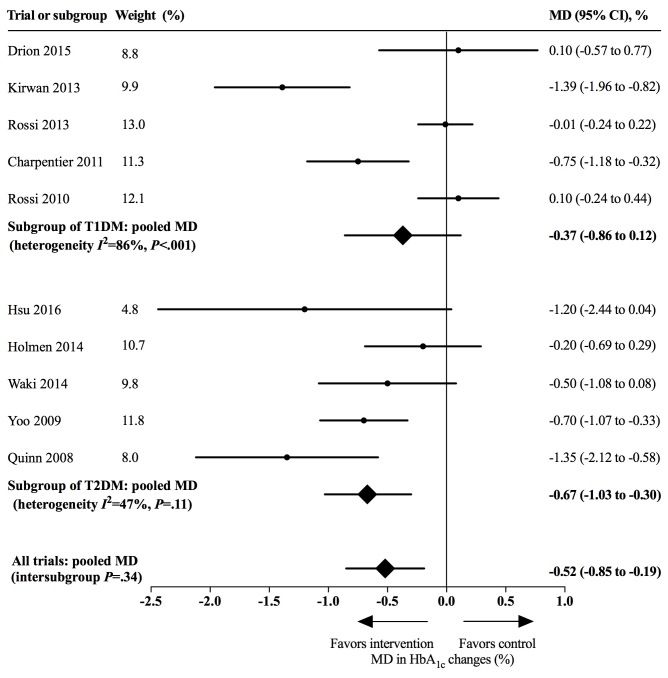
Across 12 included trials involving 974 participants, using app-based interventions was associated with a clinically significant reduction of HbA (MD 0.48%, 95% CI 0.19%-0.77%) without excess adverse events. Larger HbA reductions were noted among patients with type 2 diabetes than those with type 1 diabetes (MD 0.67%, 95% CI 0.30%-1.03% vs MD 0.36%, 95% CI 0.08%-0.81%). Having a complication prevention module in app-based interventions was associated with a greater HbA reduction (with complication prevention: MD 1.31%, 95% CI 0.66%-1.96% vs without: MD 0.38%, 95% CI 0.09%-0.67%; intersubgroup P=.01), as was having a structured display (with structured display: MD 0.69%, 95% CI 0.32%-1.06% vs without: MD 0.16%, 95% CI 0.16%-0.48%; intersubgroup P=.03). However, having a clinical decision-making function was not associated with a larger HbA reduction (with clinical decision making: MD 0.18%, 95% CI 0.21%-0.56% vs without: MD 0.61%, 95% CI 0.27%-0.95%; intersubgroup P=.10).
The use of mobile app-based interventions yields a clinically significant HbA reduction among adult outpatients with diabetes, especially among those with type 2 diabetes. Our study suggests that the clinical decision-making function needs further improvement and evaluation before being added to apps.
用于糖尿病自我管理的移动健康应用程序具有不同的功能。然而,每种功能的疗效和安全性尚未得到充分研究,且这些功能尚无分类。
本研究的目的是:(1)开发并验证糖尿病自我管理应用程序的分类法;(2)在一项随机对照试验(RCT)的系统评价中,调查基于移动应用程序的干预措施对成年糖尿病患者的血糖疗效;(3)使用该分类法探索不同功能对基于应用程序的整体干预效果的贡献。
我们开发了一个三轴分类法,其列代表临床模块,行代表功能模块,单元格代表带有风险评估的功能。通过对市售糖尿病应用程序进行审查和分类来验证该分类法。我们检索了2007年1月至2016年5月期间的MEDLINE、EMBASE、Cochrane对照试验中央注册库、中国生物医学文献数据库和ClinicalTrials.gov。我们纳入了成年糖尿病门诊患者的RCT,这些试验比较了使用基于移动应用程序的干预措施与单纯常规护理。使用随机效应荟萃分析汇总血红蛋白A(HbA)浓度的平均差异(MDs)和不良事件的风险比。在进行分类后,我们对纳入的基于应用程序的干预措施中每个模块的有无进行了探索性亚组分析。
在纳入的涉及974名参与者的12项试验中,使用基于应用程序的干预措施与HbA临床显著降低相关(MD 0.48%,95%CI 0.19%-0.77%),且无过多不良事件。2型糖尿病患者的HbA降低幅度大于1型糖尿病患者(MD 0.67%,95%CI 0.30%-1.03%对比MD 0.36%,95%CI 0.08%-0.81%)。基于应用程序的干预措施中具有并发症预防模块与更大的HbA降低相关(有并发症预防:MD 1.31%,95%CI 0.66%-1.96%对比无:MD 0.38%,95%CI 0.09%-0.67%;亚组间P=0.01),具有结构化显示也是如此(有结构化显示:MD 0.69%,95%CI 0.32%-1.06%对比无:MD 0.16%,95%CI 0.16%-0.48%;亚组间P=0.03)。然而,具有临床决策功能与更大的HbA降低无关(有临床决策:MD 0.18%,95%CI 0.21%-0.56%对比无:MD 0.61%,95%CI 0.27%-0.95%;亚组间P=0.10)。
使用基于移动应用程序的干预措施可使成年糖尿病门诊患者的HbA临床显著降低,尤其是2型糖尿病患者。我们的研究表明,临床决策功能在添加到应用程序之前需要进一步改进和评估。