Lule Swaib A, Mpairwe Harriet, Nampijja Margaret, Akello Florence, Kabagenyi Joyce, Namara Benigna, Nkurunungi Gyaviira, Kizito Dennison, Kahwa Joseph, Muhangi Lawrence, Nash Stephen, Muwanga Moses, Webb Emily L, Elliott Alison M
London School of Hygiene and Tropical Medicine, London, UK.
MRC/UVRI Uganda Research Unit, Entebbe, Uganda.
Pediatr Allergy Immunol. 2017 Jun;28(4):377-383. doi: 10.1111/pai.12719.
In high-income countries, allergy-related diseases (ARDs) follow a typical sequence, the 'Atopic March'. Little is known about the life-course of ARDs in the markedly different, low-income, tropical environment. We describe ARDs in a tropical, African birth cohort.
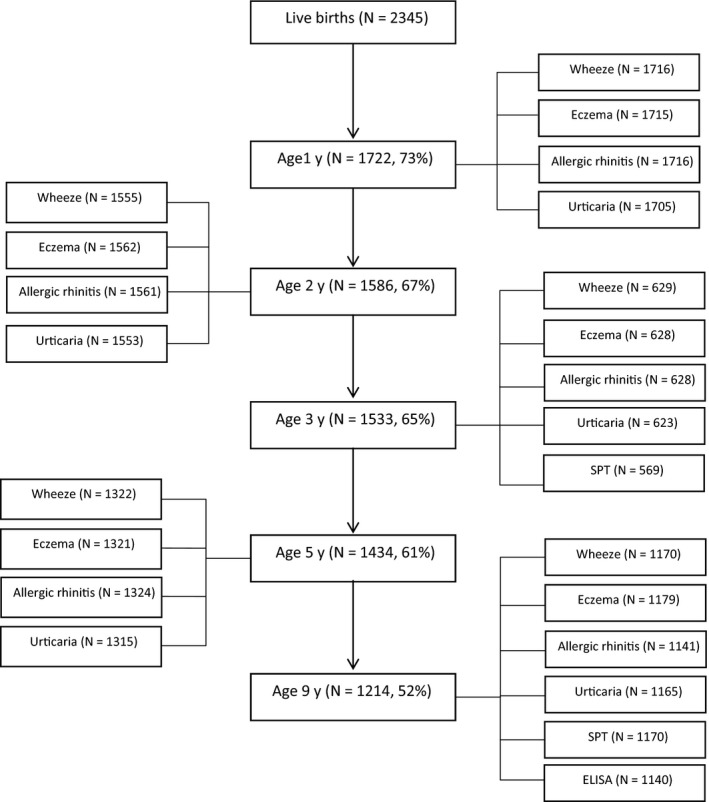
Ugandan children were followed from birth to 9 years. ISAAC questionnaires were completed at intervals; doctor-diagnosed ARDs were recorded throughout follow-up. Skin prick tests (SPTs) were performed at 3 and 9 years. Atopy was defined as ≥1 positive SPT.
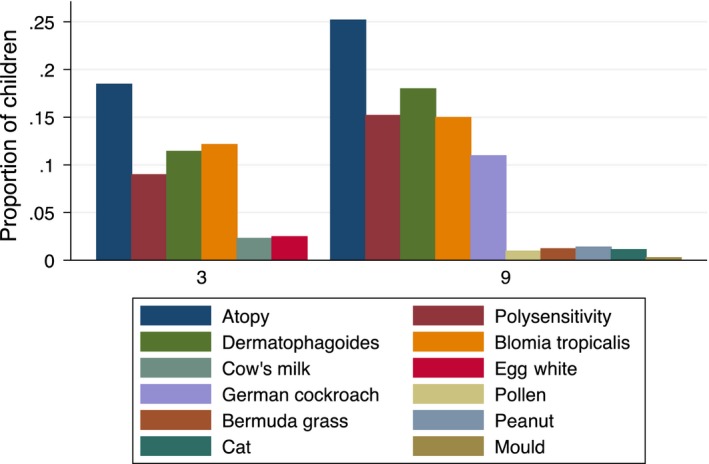
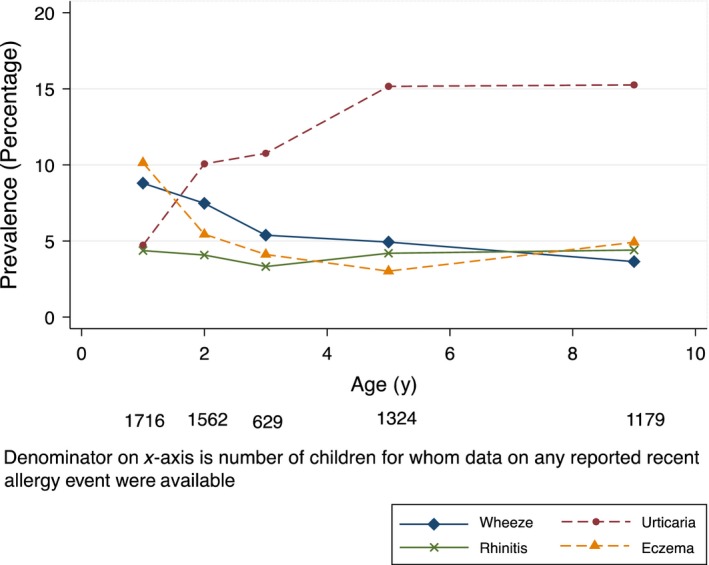
Of the 2345 live-born children, 1214 (52%) were seen at 9 years. Wheeze and eczema were common in infancy, but by 9 years, only 4% reported recent wheeze, 5% eczema and 5% rhinitis. Between 3 and 9 years, atopy prevalence increased from 19% to 25%. Atopy at 3 or 9 years was associated with reported ARD events at 9 years, for example OR = 5.2 (95% CI 2.9-10.7) for atopy and recent wheeze at 9 years. Reported or doctor-diagnosed ARD events in early childhood were associated with the same events in later childhood, for example OR = 4.4 (2.3-8.4) for the association between reported wheeze before 3 years with reported recent wheeze at 9 years, but progression from early eczema to later rhinitis or asthma was not observed.
Allergen sensitization started early in childhood and increased with age. Eczema and wheeze were common in infancy and declined with age. Atopy was strongly associated with ARD among the few affected children. The typical Atopic March did not occur. Environmental exposures during childhood may dissociate atopy and ARD.
在高收入国家,过敏相关疾病(ARDs)遵循典型的顺序,即“特应性进程”。对于在明显不同的低收入热带环境中ARDs的生命历程知之甚少。我们描述了一个热带非洲出生队列中的ARDs情况。
乌干达儿童从出生起被随访至9岁。定期完成国际儿童哮喘和过敏研究(ISAAC)问卷;在整个随访过程中记录医生诊断的ARDs。在3岁和9岁时进行皮肤点刺试验(SPT)。特应性定义为SPT结果≥1项为阳性。
在2345名活产儿童中,9岁时对1214名(52%)进行了观察。喘息和湿疹在婴儿期很常见,但到9岁时,只有4%的儿童报告近期有喘息,5%有湿疹,5%有鼻炎。在3岁至9岁之间,特应性患病率从19%升至25%。3岁或9岁时的特应性与9岁时报告的ARD事件相关,例如9岁时特应性与近期喘息的比值比(OR)=5.2(95%置信区间2.9 - 10.7)。儿童早期报告的或医生诊断的ARD事件与儿童后期的相同事件相关,例如3岁前报告的喘息与9岁时报告的近期喘息之间的关联的OR = 4.4(2.3 - 8.4),但未观察到从早期湿疹进展为后期鼻炎或哮喘的情况。
过敏原致敏在儿童早期开始并随年龄增加。湿疹和喘息在婴儿期很常见且随年龄下降。在少数受影响的儿童中,特应性与ARD密切相关。典型的特应性进程未出现。儿童期的环境暴露可能使特应性和ARD分离。