Kirk Paul, Sheppard Mary, Carpenter John-Paul, Anderson Lisa, He Taigang, St Pierre Tim, Galanello Renzo, Catani Gualtiero, Wood John, Fucharoen Suthat, Porter John B, Walker J Malcolm, Forni Gian Luca, Pennell Dudley J
Cardiovascular Magnetic Resonance Unit, Royal Brompton Hospital, Sydney Street, SW3 6NP, London, UK.
National Heart and Lung Institute, Imperial College, London, UK.
J Cardiovasc Magn Reson. 2017 Mar 27;19(1):36. doi: 10.1186/s12968-017-0349-3.
Heart failure related to cardiac siderosis remains a major cause of death in transfusion dependent anaemias. Replacement fibrosis has been reported as causative of heart failure in siderotic cardiomyopathy in historical reports, but these findings do not accord with the reversible nature of siderotic heart failure achievable with intensive iron chelation.
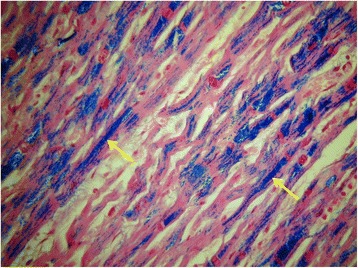
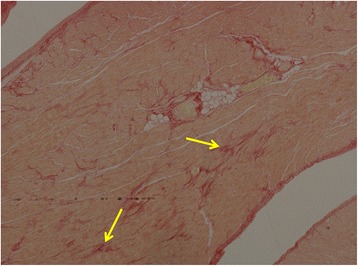
Ten whole human hearts (9 beta-thalassemia major, 1 sideroblastic anaemia) were examined for iron loading and fibrosis (replacement and interstitial). Five had died from heart failure, 4 had cardiac transplantation for heart failure, and 1 had no heart failure (death from a stroke). Heart samples iron content was measured using atomic emission spectroscopy. Interstitial fibrosis was quantified by computer using picrosirius red (PSR) staining and expressed as collagen volume fraction (CVF) with normal value for left ventricle <3%.
The 9 hearts affected by heart failure had severe iron loading with very low T2* of 5.0 ± 2.0 ms (iron concentration 8.5 ± 7.0 mg/g dw) and diffuse granular myocardial iron deposition. In none of the 10 hearts was significant macroscopic replacement fibrosis present. In only 2 hearts was interstitial fibrosis present, but with low CVF: in one patient with no cardiac siderosis (death by stroke, CVF 5.9%) and in a heart failure patient (CVF 2%). In the remaining 8 patients, no interstitial fibrosis was seen despite all having severe cardiac siderosis and heart failure (CVF 1.86% ±0.87%).
Replacement cardiac fibrosis was not seen in the 9 post-mortem hearts from patients with severe cardiac siderosis and heart failure leading to death or transplantation, which contrasts markedly to historical reports. Minor interstitial fibrosis was also unusual and very limited in extent. These findings accord with the potential for reversibility of heart failure seen in iron overload cardiomyopathy.
ClinicalTrials.gov Identifier: NCT00520559.
与心脏铁沉积相关的心力衰竭仍然是依赖输血的贫血症患者的主要死因。在既往报告中,替代性纤维化被认为是铁沉着性心肌病心力衰竭的病因,但这些发现与强化铁螯合治疗可实现的铁沉着性心力衰竭的可逆性不符。
对10例完整的人体心脏(9例重型β地中海贫血、1例铁粒幼细胞贫血)进行铁负荷和纤维化(替代性和间质纤维化)检查。其中5例死于心力衰竭,4例因心力衰竭接受心脏移植,1例无心力衰竭(死于中风)。采用原子发射光谱法测量心脏样本的铁含量。使用苦味酸天狼星红(PSR)染色通过计算机对间质纤维化进行定量,并表示为胶原容积分数(CVF),左心室正常值<3%。
9例受心力衰竭影响的心脏有严重的铁负荷,T2*极低,为5.0±2.0毫秒(铁浓度8.5±7.0毫克/克干重),心肌铁呈弥漫性颗粒状沉积。10例心脏中均未出现明显的宏观替代性纤维化。仅2例心脏存在间质纤维化,但CVF较低:1例无心脏铁沉积的患者(死于中风,CVF为5.9%)和1例心力衰竭患者(CVF为2%)。其余8例患者尽管均有严重的心脏铁沉积和心力衰竭,但未见间质纤维化(CVF为1.86%±0.87%)。
在9例因严重心脏铁沉积和心力衰竭导致死亡或接受移植的患者的尸检心脏中未发现替代性心脏纤维化,这与既往报告形成明显对比。轻微的间质纤维化也不常见且程度非常有限。这些发现与铁过载心肌病中心力衰竭的可逆性潜力相符。
ClinicalTrials.gov标识符:NCT00520559。