Lin Yu-Hsiang, Hou Chen-Pang, Chen Tien-Hsing, Juang Horng-Heng, Chang Phei-Lang, Yang Pei-Shan, Lin Yu-Sheng, Chen Chien-Lun, Tsui Ke-Hung
Department of Urology, Chang Gung Memorial Hospital - Linkou; School of Medicine; Graduate Institute of Clinical Medical Sciences, College of Medicine, Chang Gung University.
Department of Urology, Chang Gung Memorial Hospital - Linkou; School of Medicine.
Clin Interv Aging. 2017 Mar 16;12:535-541. doi: 10.2147/CIA.S126207. eCollection 2017.
We assessed the lower urinary tract symptoms (LUTSs) and clinical outcomes between diabetes mellitus (DM) patients and non-diabetic (non-DM) patients receiving transurethral resection of prostate (TUR-P).
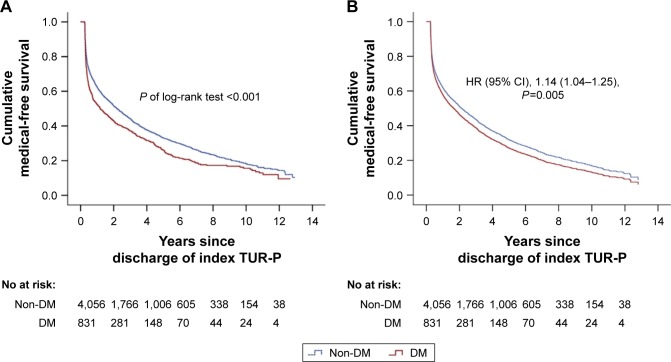
This analysis was a retrospective cohort study using 13 years (2000-2012) of claims data from Taiwan's National Health Insurance Research Database (NHIRD). A total of 4,887 patients who had persistent LUTSs and underwent TUR-P for prostate enlargement (benign prostate enlargement [BPE]) were enrolled and divided into two groups: DM and non-DM groups. The patients' characteristics, postoperative clinical outcomes, and the medication records after TUR-P were compared. Chi-square test was used for categorical variables and independent samples -test for continuous variables. Multivariable logistic regression analysis was used to compare the risk of postoperative outcomes. Finally, we estimated the medication-free survival rate after TUR-P using Kaplan-Meier method and compared it between study groups using log-rank test.
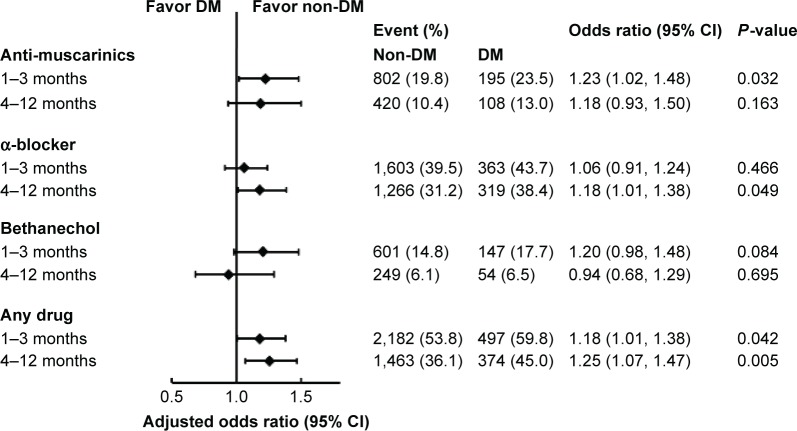
DM group patients had a higher prevalence of comorbidities. Postoperatively, the DM group had lower rates of urinary tract infection (UTI; odds ratio [OR], 0.78; =0.009) and higher rates of urinary retention requiring catheterization (OR, 1.35; =0.01) within 1 month after TUR-P. A higher proportion of patients with DM took anti-muscarinics (OR, 1.23; =0.032) within the first 3 months and α-blockers (OR, 1.18; =0.049) during 3-12 months after receiving TUR-P. Overall, the DM group patients had a worse postoperative medication-free survival compared to that of non-DM group patients (95% confidence interval [95% CI], 1.14; =0.005).
DM patients require higher rates of continuing medication after TUR-P, especially anti-muscarinics in 3 months postoperatively and alpha-blocker after 3 months postoperatively. DM patients also had higher incidence of urine retention after surgery. DM patients had relatively poor treatment outcomes compared to DM-free patients.
我们评估了糖尿病(DM)患者与接受经尿道前列腺切除术(TUR-P)的非糖尿病(非DM)患者的下尿路症状(LUTS)及临床结局。
本分析是一项回顾性队列研究,使用了来自台湾国民健康保险研究数据库(NHIRD)的13年(2000 - 2012年)索赔数据。共有4887例患有持续性LUTS且因前列腺增生(良性前列腺增生[BPE])接受TUR-P的患者被纳入研究,并分为两组:DM组和非DM组。比较了患者的特征、术后临床结局以及TUR-P后的用药记录。分类变量采用卡方检验,连续变量采用独立样本t检验。多变量逻辑回归分析用于比较术后结局的风险。最后,我们使用Kaplan-Meier方法估计TUR-P后的无药生存率,并使用对数秩检验在研究组之间进行比较。
DM组患者合并症的患病率更高。术后,DM组在TUR-P后1个月内尿路感染(UTI)发生率较低(比值比[OR],0.78;P = 0.009),而需要导尿的尿潴留发生率较高(OR,1.35;P = 0.01)。更高比例的DM患者在接受TUR-P后的前3个月内服用抗毒蕈碱药物(OR,1.23;P = 0.032),在3至12个月期间服用α受体阻滞剂(OR,1.18;P = 0.049)。总体而言,与非DM组患者相比,DM组患者术后的无药生存率更差(95%置信区间[95%CI],1.14;P = 0.005)。
DM患者在TUR-P后需要更高比例的持续用药,尤其是术后3个月内的抗毒蕈碱药物和术后3个月后的α受体阻滞剂。DM患者术后尿潴留的发生率也更高。与无DM患者相比,DM患者的治疗结局相对较差。