Kosack Cara S, Page Anne-Laure, Beelaert Greet, Benson Tumwesigye, Savane Aboubacar, Ng'ang'a Anne, Andre Bita, Zahinda Jean-Paul Bn, Shanks Leslie, Fransen Katrien
Médecins sans Frontières, Diagnostic Network, Amsterdam, Netherlands.
Epicentre, Epidemiology and Population Health Department, Paris, France.
J Int AIDS Soc. 2017 Mar 24;19(1):21345. doi: 10.7448/IAS.20.1.21345.
Although individual HIV rapid diagnostic tests (RDTs) show good performance in evaluations conducted by WHO, reports from several African countries highlight potentially significant performance issues. Despite widespread use of RDTs for HIV diagnosis in resource-constrained settings, there has been no systematic, head-to-head evaluation of their accuracy with specimens from diverse settings across sub-Saharan Africa. We conducted a standardized, centralized evaluation of eight HIV RDTs and two simple confirmatory assays at a WHO collaborating centre for evaluation of HIV diagnostics using specimens from six sites in five sub-Saharan African countries.
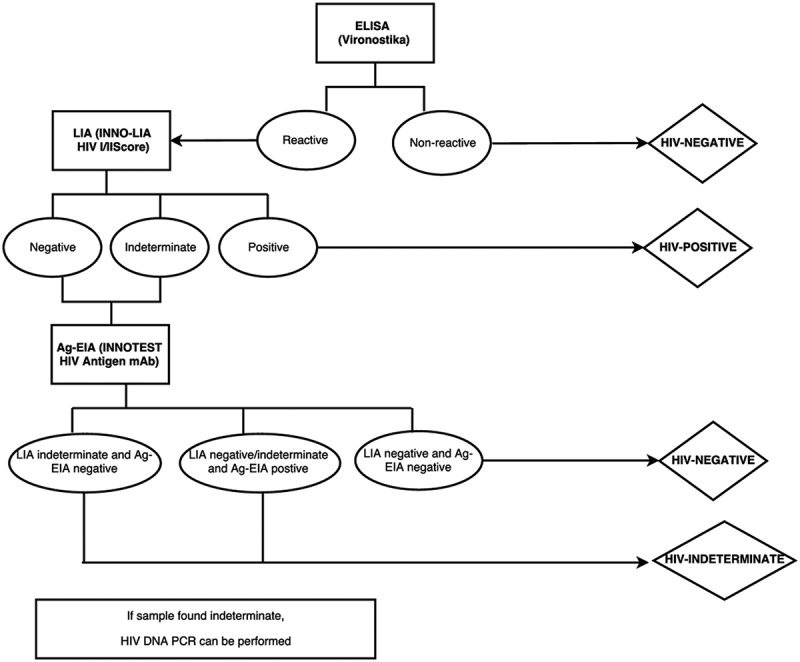
Specimens were transported to the Institute of Tropical Medicine (ITM), Antwerp, Belgium for testing. The tests were evaluated by comparing their results to a state-of-the-art reference algorithm to estimate sensitivity, specificity and predictive values.
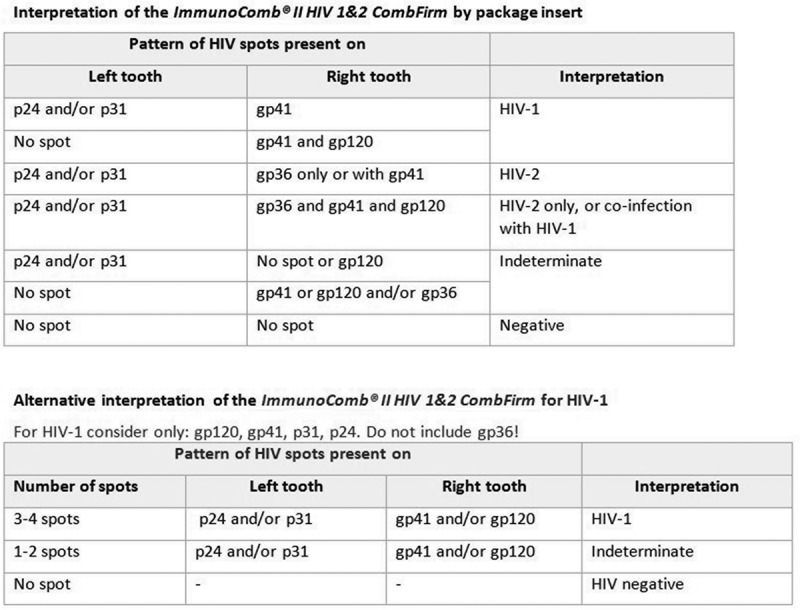
2785 samples collected from August 2011 to January 2015 were tested at ITM. All RDTs showed very high sensitivity, from 98.8% for First Response HIV Card Test 1-2.0 to 100% for Determine HIV 1/2, Genie Fast, SD Bioline HIV 1/2 3.0 and INSTI HIV-1/HIV-2 Antibody Test kit. Specificity ranged from 90.4% for First Response to 99.7% for HIV 1/2 STAT-PAK with wide variation based on the geographical origin of specimens. Multivariate analysis showed several factors were associated with false-positive results, including gender, provider-initiated testing and the geographical origin of specimens. For simple confirmatory assays, the total sensitivity and specificity was 100% and 98.8% for ImmunoComb II HIV 12 CombFirm (ImmunoComb) and 99.7% and 98.4% for Geenius HIV 1/2 with indeterminate rates of 8.9% and 9.4%.
In this first systematic head-to-head evaluation of the most widely used RDTs, individual RDTs performed more poorly than in the WHO evaluations: only one test met the recommended thresholds for RDTs of ≥99% sensitivity and ≥98% specificity. By performing all tests in a centralized setting, we show that these differences in performance cannot be attributed to study procedure, end-user variation, storage conditions, or other methodological factors. These results highlight the existence of geographical and population differences in individual HIV RDT performance and underscore the challenges of designing locally validated algorithms that meet the latest WHO-recommended thresholds.
尽管个体HIV快速诊断检测(RDT)在世卫组织开展的评估中表现良好,但来自几个非洲国家的报告突出了潜在的重大性能问题。尽管RDT在资源有限的环境中被广泛用于HIV诊断,但尚未对其在撒哈拉以南非洲不同地区标本的准确性进行系统的、直接的评估。我们在世卫组织一个HIV诊断评估合作中心,使用来自撒哈拉以南非洲五个国家六个地点的标本,对八种HIV RDT和两种简单确证检测进行了标准化的集中评估。
标本被运至比利时安特卫普的热带医学研究所(ITM)进行检测。通过将检测结果与一种先进的参考算法进行比较来评估这些检测,以估计敏感性、特异性和预测值。
2011年8月至20l5年1月收集的2785份样本在ITM进行了检测。所有RDT均显示出非常高的敏感性,从First Response HIV Card Test 1 - 2.0的98.8%到Determine HIV 1/2、Genie Fast、SD Bioline HIV 1/2 3.0和INSTI HIV - 1/HIV - 2抗体检测试剂盒的100%。特异性从First Response的90.4%到HIV 1/2 STAT - PAK的99.7%不等,基于标本的地理来源存在很大差异。多变量分析显示,包括性别、提供者发起的检测和标本的地理来源在内的几个因素与假阳性结果相关。对于简单确证检测,ImmunoComb II HIV 12 CombFirm(ImmunoComb)的总敏感性和特异性分别为100%和98.8%;Geenius HIV 1/2的总敏感性和特异性分别为99.7%和98.4%,不确定率分别为8.9%和9.4%。
在这次对最广泛使用的RDT首次进行的系统直接评估中,单个RDT的表现比在世卫组织评估中更差:只有一种检测达到了RDT推荐的阈值,即敏感性≥99%和特异性≥98%。通过在集中环境中进行所有检测,我们表明这些性能差异不能归因于研究程序、终端用户差异、储存条件或其他方法学因素。这些结果突出了个体HIV RDT性能存在地理和人群差异,并强调了设计符合世卫组织最新推荐阈值的本地验证算法所面临的挑战。