Bernstein Jonathan A, Cremonesi Paolo, Hoffmann Thomas K, Hollingsworth John
Division of Immunology/Allergy, University of Cincinnati, 231 Albert Sabin Way, Cincinnati, OH, 45267, USA.
Department of Emergency Medicine, E. O. Galliera Hospital, Genoa, Italy.
Int J Emerg Med. 2017 Dec;10(1):15. doi: 10.1186/s12245-017-0141-z. Epub 2017 Apr 13.
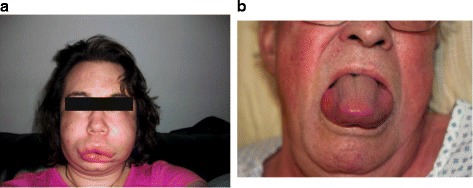
Angioedema is a common presentation in the emergency department (ED). Airway angioedema can be fatal; therefore, prompt diagnosis and correct treatment are vital.
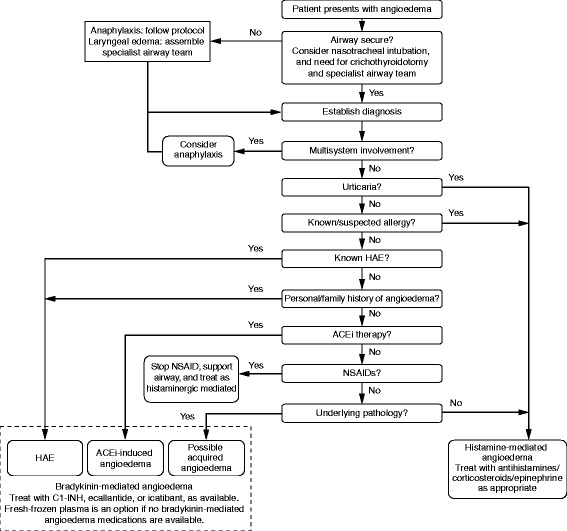
Based on the findings of two expert panels attended by international experts in angioedema and emergency medicine, this review aims to provide practical guidance on the diagnosis, differentiation, and management of histamine- and bradykinin-mediated angioedema in the ED.
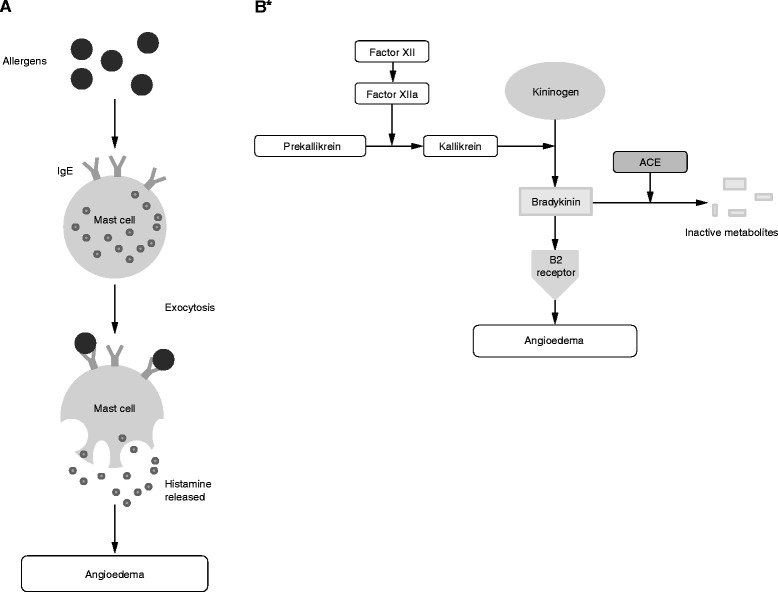
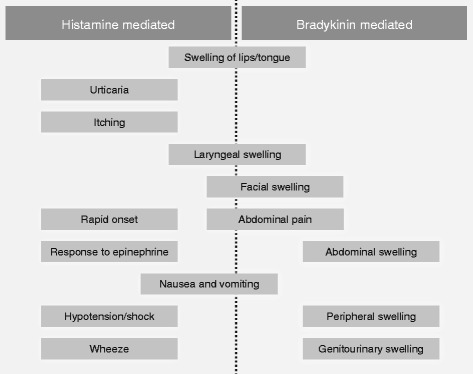
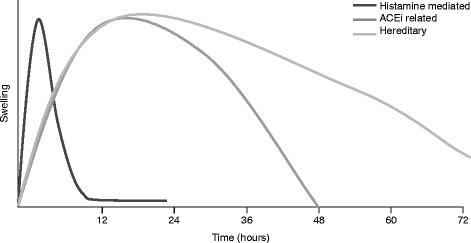
The most common pathophysiology underlying angioedema is mediated by histamine; however, ED staff must be alert for the less common bradykinin-mediated forms of angioedema. Crucially, bradykinin-mediated angioedema does not respond to the same treatment as histamine-mediated angioedema. Bradykinin-mediated angioedema can result from many causes, including hereditary defects in C1 esterase inhibitor (C1-INH), side effects of angiotensin-converting enzyme inhibitors (ACEis), or acquired deficiency in C1-INH. The increased use of ACEis in recent decades has resulted in more frequent encounters with ACEi-induced angioedema in the ED; however, surveys have shown that many ED staff may not know how to recognize or manage bradykinin-mediated angioedema, and hospitals may not have specific medications or protocols in place.
ED physicians must be aware of the different pathophysiologic pathways that lead to angioedema in order to efficiently and effectively manage these potentially fatal conditions.
血管性水肿是急诊科常见的病症表现。气道血管性水肿可能会致命;因此,及时诊断和正确治疗至关重要。
基于血管性水肿和急诊医学领域国际专家参加的两个专家小组的研究结果,本综述旨在为急诊科组胺和缓激肽介导的血管性水肿的诊断、鉴别及管理提供实用指导。
血管性水肿最常见的病理生理机制是由组胺介导;然而,急诊科工作人员必须警惕较不常见的缓激肽介导的血管性水肿形式。至关重要的是,缓激肽介导的血管性水肿对组胺介导的血管性水肿的治疗反应不同。缓激肽介导的血管性水肿可由多种原因引起,包括C1酯酶抑制剂(C1-INH)的遗传性缺陷、血管紧张素转换酶抑制剂(ACEi)的副作用或C1-INH的后天性缺乏。近几十年来ACEi使用的增加导致急诊科更频繁地遇到ACEi诱导的血管性水肿;然而,调查显示许多急诊科工作人员可能不知道如何识别或处理缓激肽介导的血管性水肿,医院可能也没有特定的药物或方案。
急诊科医生必须了解导致血管性水肿的不同病理生理途径,以便有效管理这些潜在的致命病症。