Manfrin Andrea, Tinelli Michela, Thomas Trudy, Krska Janet
Medway School of Pharmacy, Universities of Greenwich and Kent at Medway, Anson Building, Central Avenue, Chatham Maritime, Chatham, Kent, ME4 4TB, UK.
LSE Health and Social Care, The London School of Economics and Political Science, Houghton Street, London, WC2A 2AE, UK.
BMC Health Serv Res. 2017 Apr 24;17(1):300. doi: 10.1186/s12913-017-2245-9.
The economic burden of asthma, which relates to the degree of control, is €5 billion annually in Italy. Pharmacists could help improve asthma control, reducing this burden. This study aimed to evaluate the effectiveness and cost-effectiveness of Medicines Use Reviews provided by community pharmacists in asthma.
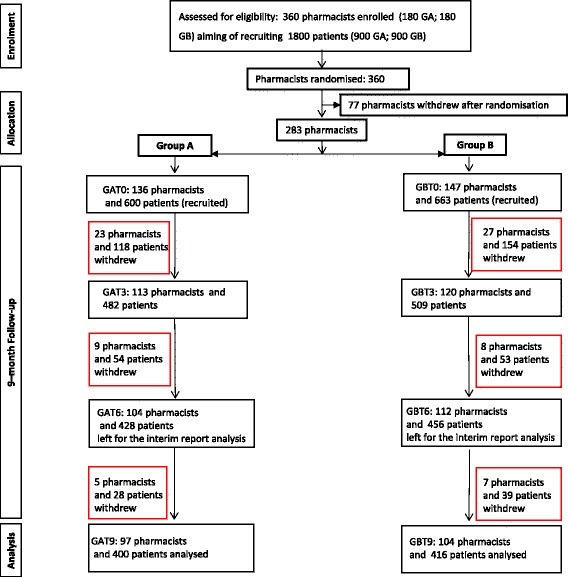
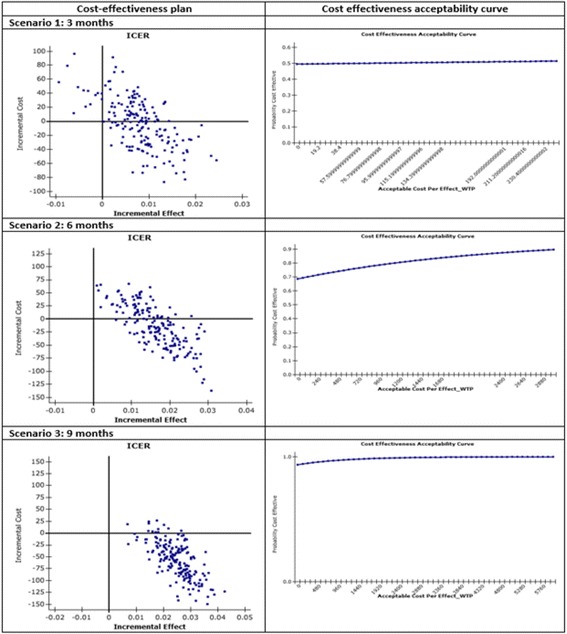
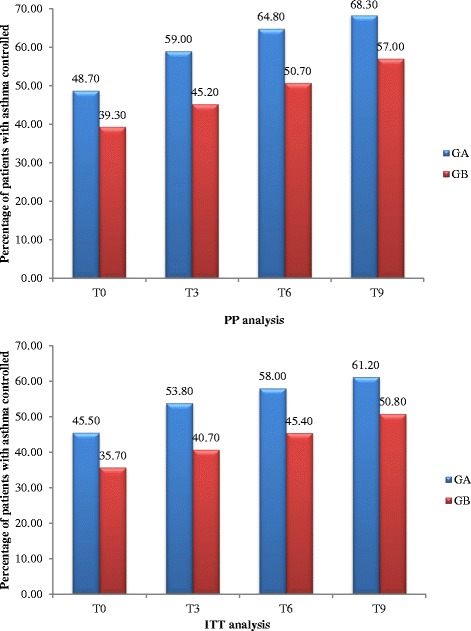
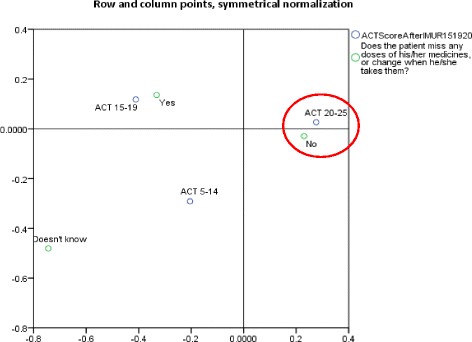
This cluster randomised, multi-centre, controlled trial in adult patients with asthma was conducted in 15 of the 20 regions of Italy between September 2014 and July 2015. After stratification by region, community pharmacists were randomly allocated to group A (trained in and delivered the intervention at baseline) or B (training and delivery 3 months later), using computerised random number generation in blocks of 10. Each recruited up to five patients, with both groups followed for 9 months. The intervention consisted of a systematic, structured face-to-face consultation with a pharmacist, covering asthma symptoms, medicines used, attitude towards medicines and adherence, recording pharmacist-identified pharmaceutical care issues (PCIs). The primary outcome was asthma control, assessed using the Asthma-Control-Test (ACT) score (ACT ≥ 20 represents good control). Secondary outcomes were: number of active ingredients, adherence, cost-effectiveness compared with usual care. Although blinding was not possible for either pharmacists or patients, assessment of outcomes was conducted by researchers blind to group allocation.
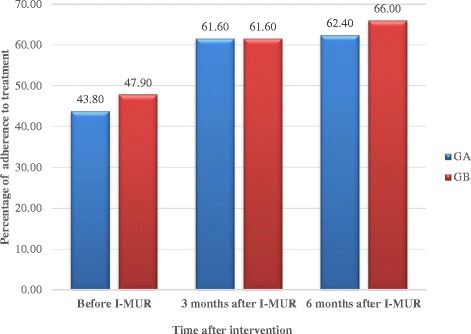
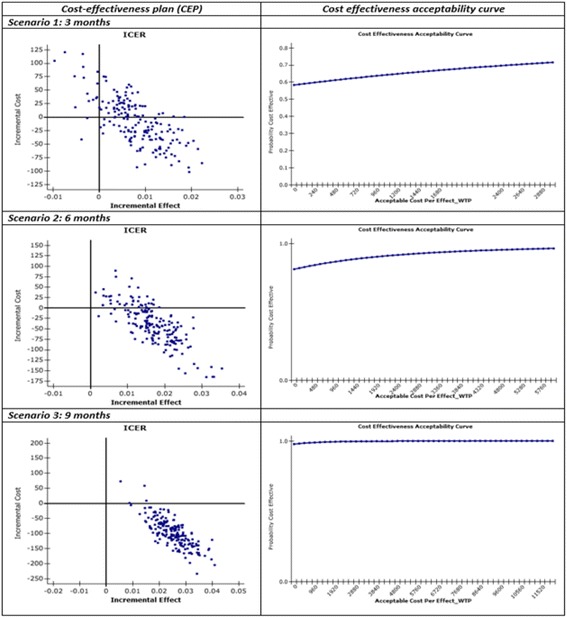
Numbers of pharmacists and patients enrolled were 283 (A = 136; B = 147) and 1263 (A = 600; B = 663), numbers completing were 201 (A = 97; B = 104) and 816 (A = 400; B = 416), respectively. Patients were similar in age and gender and 56.13% (458/816) had poor/partial asthma control. Pharmacists identified 1256 PCIs (mean 1.54/patient), mostly need for education, monitoring and potentially ineffective therapy. Median ACT score at baseline differed between groups (A = 19, B = 18; p < 0.01). Odds ratio for improved asthma control was 1.76 (95% CI 1.33-2.33) and number needed to treat 10 (95% CI 6-28). Number of active ingredients reduced by 7.9% post-intervention (p < 0.01). Adherence improved by 35.4% 3 months post-intervention and 40.0% at 6 months (p < 0.01). The probability of the intervention being more cost-effective than usual care was 100% at 9 months.
This community pharmacist-based intervention demonstrated both effectiveness and cost-effectiveness. It has since been implemented as the first community pharmacy cognitive service in Italy.
TRN: ISRCTN72438848 (registered 5 January 2015, retrospectively).
在意大利,哮喘的经济负担与控制程度相关,每年达50亿欧元。药剂师有助于改善哮喘控制,减轻这一负担。本研究旨在评估社区药剂师提供的药物使用评估在哮喘治疗中的有效性和成本效益。
2014年9月至2015年7月期间,在意大利20个地区中的15个地区,针对成年哮喘患者开展了这项整群随机、多中心对照试验。按地区分层后,使用计算机随机数生成器以10个为一组,将社区药剂师随机分配到A组(在基线时接受培训并实施干预)或B组(3个月后进行培训和实施干预)。每组最多招募5名患者,两组均随访9个月。干预措施包括与药剂师进行系统、结构化的面对面咨询,涵盖哮喘症状、所用药物、对药物的态度和依从性,记录药剂师确定的药学服务问题(PCI)。主要结局为哮喘控制情况,采用哮喘控制测试(ACT)评分进行评估(ACT≥20表示控制良好)。次要结局包括:活性成分数量、依从性、与常规治疗相比的成本效益。尽管药剂师和患者均无法设盲,但由对分组情况不知情的研究人员对结局进行评估。
纳入的药剂师和患者数量分别为283名(A组 = 136名;B组 = 147名)和1263名(A组 = 600名;B组 = 663名),完成试验的分别为201名(A组 = 97名;B组 = 104名)和816名(A组 = 400名;B组 = 416名)。患者的年龄和性别相似,56.13%(458/816)的患者哮喘控制不佳/部分控制。药剂师确定了1256个药学服务问题(平均每名患者1.54个),主要是需要教育、监测和可能无效的治疗。两组基线时的ACT评分中位数不同(A组 = 19,B组 = 18;p < 0.01)。哮喘控制改善的比值比为1.76(95%置信区间1.33 - 2.33),需治疗人数为10(95%置信区间6 - 28)。干预后活性成分数量减少了7.9%(p < 0.01)。干预后3个月依从性提高了35.4%,6个月时提高了40.0%(p < 0.01)。9个月时干预措施比常规治疗更具成本效益的概率为100%。
这项基于社区药剂师的干预措施显示出有效性和成本效益。此后,该措施已作为意大利首个社区药房认知服务得以实施。
TRN:ISRCTN72438848(2015年1月5日注册,追溯性)