Harnack Lisa J, Cogswell Mary E, Shikany James M, Gardner Christopher D, Gillespie Cathleen, Loria Catherine M, Zhou Xia, Yuan Keming, Steffen Lyn M
From Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis (L.J.H., X.Z., L.M.S.); Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, GA (M.E.C., C.G., K.Y.); Division of Preventive Medicine, Department of Medicine, University of Alabama at Birmingham (J.M.S.); Stanford Prevention Center, School of Medicine, Stanford University, Palo Alto, CA (C.D.G.); and National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD (C.M.L.).
Circulation. 2017 May 9;135(19):1775-1783. doi: 10.1161/CIRCULATIONAHA.116.024446.
Most US adults consume excess sodium. Knowledge about the dietary sources of sodium intake is critical to the development of effective reduction strategies.
A total of 450 adults were recruited from 3 geographic locations: Birmingham, AL (n=150); Palo Alto, CA (n=150); and the Minneapolis-St. Paul, MN (n=150), metropolitan areas. Equal numbers of women and men from each of 4 race/ethnic groups (blacks, Asians, Hispanics, and non-Hispanic whites) were targeted for recruitment. Four record-assisted 24-hour dietary recalls were collected from each participant with special procedures, which included the collection of duplicate samples of salt added to food at the table and in home food preparation.
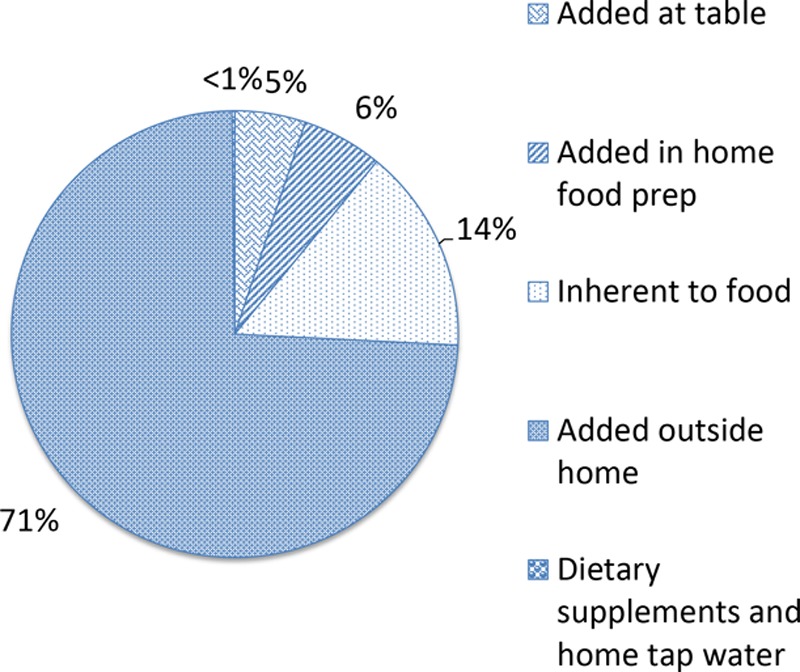
Sodium added to food outside the home was the leading source of sodium, accounting for more than two thirds (70.9%) of total sodium intake in the sample. Although the proportion of sodium from this source was smaller in some subgroups, it was the leading contributor for all subgroups. Contribution ranged from 66.3% for those with a high school level of education or less to 75.0% for those 18 to 29 years of age. Sodium inherent to food was the next highest contributor (14.2%), followed by salt added in home food preparation (5.6%) and salt added to food at the table (4.9%). Home tap water consumed as a beverage and dietary supplement and nonprescription antacids contributed minimally to sodium intake (<0.5% each).
Sodium added to food outside the home accounted for ≈70% of dietary sodium intake. This finding is consistent with the 2010 Institute of Medicine recommendation for reduction of sodium in commercially processed foods as the primary strategy to reduce sodium intake in the United States.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT02474693.
大多数美国成年人钠摄入过量。了解钠摄入的饮食来源对于制定有效的减少策略至关重要。
从3个地理位置招募了450名成年人:阿拉巴马州伯明翰(n = 150);加利福尼亚州帕洛阿尔托(n = 150);明尼苏达州明尼阿波利斯 - 圣保罗(n = 150)的大都市区。目标是从4个种族/族裔群体(黑人、亚洲人、西班牙裔和非西班牙裔白人)中各招募同等数量的男性和女性。通过特殊程序从每位参与者收集4次记录辅助的24小时饮食回忆,其中包括收集在餐桌上和家庭食物制备中添加到食物中的盐的重复样本。
外出就餐时添加到食物中的钠是钠的主要来源,占样本中总钠摄入量的三分之二以上(70.9%)。尽管该来源的钠在某些亚组中的比例较小,但它是所有亚组的主要贡献者。贡献范围从高中及以下学历者的66.3%到18至 29岁者的75.0%。食物本身所含的钠是第二大贡献者(14.2%),其次是家庭食物制备中添加的盐(5.6%)和餐桌上添加到食物中的盐(4.9%)。作为饮料和膳食补充剂饮用的家庭自来水和非处方抗酸剂对钠摄入的贡献最小(各<0.5%)。
外出就餐时添加到食物中的钠约占膳食钠摄入量的70%。这一发现与2010年医学研究所关于减少商业加工食品中的钠作为美国减少钠摄入的主要策略的建议一致。