Botnar Research Centre, University of Oxford, Windmill Road, Oxford, OX3 7LD, UK.
Knee Surg Sports Traumatol Arthrosc. 2018 Apr;26(4):1152-1157. doi: 10.1007/s00167-017-4544-4. Epub 2017 Apr 21.
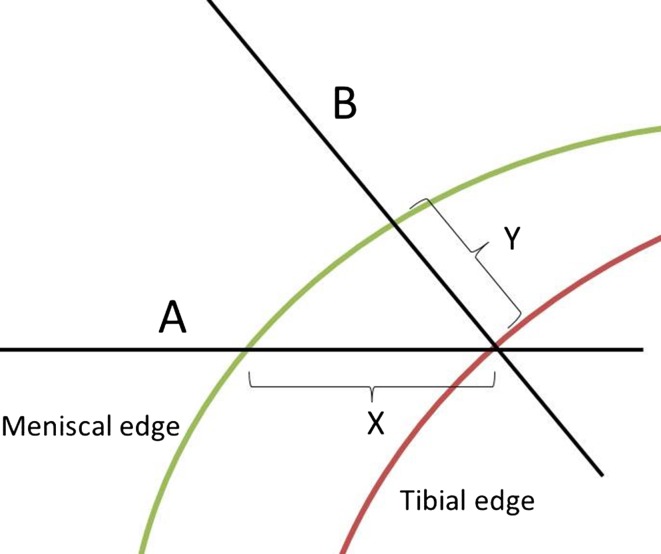
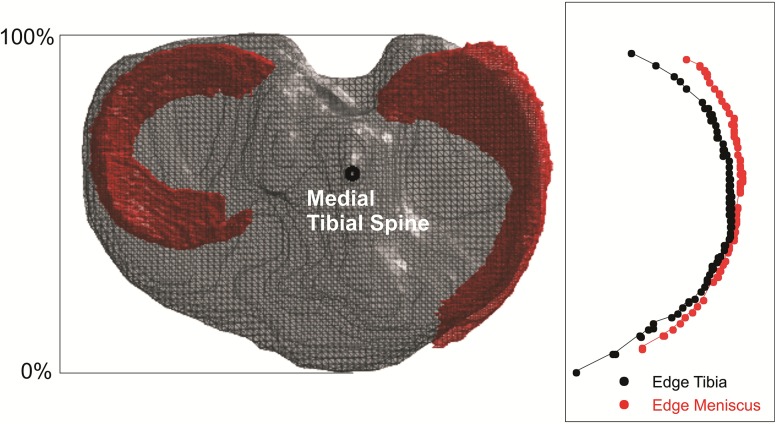
Longitudinal cohort studies of knee OA aetiology use MRI to assess meniscal extrusion within the same knee at sequential time points. A validated method of assessment is required to ensure that extrusion is measured at the same location within the knee at each time point. Absolute perpendicular extrusion from the tibial edge can be assessed using the reference standard of segmentation of the tibia and medial meniscus. This is labour intensive and unsuitable for large cohorts. Two methods are commonly used as proxy measurements. Firstly, the apex of the medial tibial spine is used to identify a reproducible MRI coronal slice, from which extrusion is measured. Secondly, the coronal MRI slice of the knee demonstrating the greatest extrusion is used. The purpose of this study was to validate these two methods against the reference standard and to determine the most appropriate method to use in longitudinal cohort studies. We hypothesised that there is no difference in absolute meniscal extrusion measurements between methods.
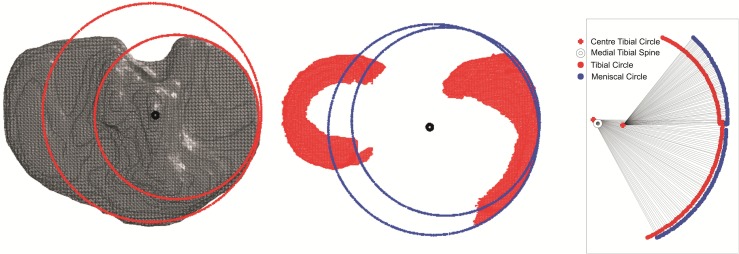
Twenty high-resolution knee MRI scans were obtained in asymptomatic subjects. The tibia and medial meniscus were manually segmented. A custom MATLAB program was used to determine the difference in medial meniscal extrusion of the knee using the reference standard compared to the two other methods.
Assessing extrusion using the single coronal MRI slice demonstrating the greatest extrusion overestimates the true extrusion of the medial meniscus. It incorrectly places the greatest meniscal extrusion at the anterior part of the tibia. Assessing extrusion using a consistent anatomical landmark, such as the medial tibial spine, most reliably corresponds to the reference of segmentation and measurement of true perpendicular extrusion from the tibial edge. Clinicians and researchers should consider this when assessing meniscal extrusion in the knee, and how it changes over time.
This study suggests measuring meniscal extrusion on the coronal MRI slice corresponding to the apex of the medial tibial spine as this correlates most closely with the true perpendicular extrusion measurements obtained from manually segmented models.
Diagnostic, Level I.
膝关节骨关节炎病因的纵向队列研究使用 MRI 来评估同一膝关节在连续时间点的半月板外突。需要一种经过验证的评估方法,以确保在每个时间点都在膝关节的同一位置测量外突。使用胫骨和内侧半月板分割的参考标准,可以评估胫骨边缘的绝对垂直外突。这是劳动密集型的,不适合大型队列。通常使用两种方法作为替代测量方法。首先,使用内侧胫骨棘的顶点来识别可重复的 MRI 冠状切片,从该切片测量外突。其次,使用显示最大外突的膝关节冠状 MRI 切片。本研究的目的是验证这两种方法与参考标准的一致性,并确定在纵向队列研究中使用最适当的方法。我们假设在绝对半月板外突测量方面,两种方法之间没有差异。
在无症状受试者中获得 20 个高分辨率膝关节 MRI 扫描。手动分割胫骨和内侧半月板。使用自定义的 MATLAB 程序,使用参考标准与另外两种方法相比,确定膝关节内侧半月板外突的差异。
使用显示最大外突的单个冠状 MRI 切片评估外突会高估内侧半月板的真实外突。它错误地将最大半月板外突放置在胫骨的前部分。使用一致的解剖学标志(如内侧胫骨棘)评估外突最可靠地对应于分割和测量胫骨边缘的真实垂直外突的参考。临床医生和研究人员在评估膝关节半月板外突及其随时间的变化时应考虑这一点。
本研究表明,在对应于内侧胫骨棘顶点的冠状 MRI 切片上测量半月板外突,因为这与从手动分割模型获得的真实垂直外突测量最密切相关。
诊断,一级。