Williamson Jeremy Stuart, Jones Huw Geraint, Williams Namor, Griffiths Anthony Paul, Jenkins Gareth, Beynon John, Harris Dean Anthony
Jeremy Stuart Williamson, Huw Geraint Jones, John Beynon, Dean Anthony Harris, Department of General and Colorectal Surgery, Singleton Hospital, Swansea SA2 8QA, United Kingdom.
World J Gastrointest Oncol. 2017 May 15;9(5):209-217. doi: 10.4251/wjgo.v9.i5.209.
To identify whether CpG island methylator phenotype (CIMP) is predictive of response to neoadjuvant chemoradiotherapy (NACRT) and outcomes in rectal cancer.
Patients undergoing NACRT and surgical resection for rectal cancer in a tertiary referral centre between 2002-2011 were identified. Pre-treatment tumour biopsies were analysed for CIMP status (high, intermediate or low) using methylation specific PCR. and status were also determined using pyrosequencing analysis. Clinical information was extracted from case records and cancer services databases. Response to radiotherapy was measured by tumour regression scores determined upon histological examination of the resected specimen. The relationship between these molecular features, response to NACRT and oncological outcomes were analysed.
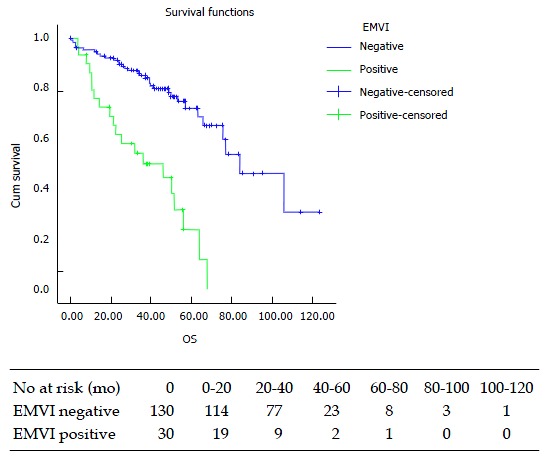
There were 160 patients analysed with a median follow-up time of 46.4 mo. Twenty-one (13%) patients demonstrated high levels of CIMP methylation (CIMP-H) and this was significantly associated with increased risk of extramural vascular invasion (EMVI) compared with CIMP-L [8/21 (38%) 15/99 (15%), = 0.028]. CIMP status was not related to tumour regression after radiotherapy or survival, however EMVI was significantly associated with adverse survival ( < 0.001). Intermediate CIMP status was significantly associated with mutation ( = 0.01). There were 14 (9%) patients with a pathological complete response (pCR) compared to 116 (73%) patients having no or minimal regression after neoadjuvant chemoradiotherapy. Those patients with pCR had median survival of 106 mo compared to 65.8 mo with minimal regression, although this was not statistically significant ( = 0.26). Binary logistic regression analysis of the relationship between EMVI and other prognostic features revealed, EMVI positivity was associated with poor overall survival, advanced "T" stage and CIMP-H but not nodal status, age, sex, mutation status and presence of local or systemic recurrence.
We report a novel association of pre-treatment characterisation of CIMP-H with EMVI status which has prognostic implications and is not readily detectable on pre-treatment histological examination.
确定CpG岛甲基化表型(CIMP)是否可预测直肠癌新辅助放化疗(NACRT)的疗效及预后。
确定2002年至2011年间在一家三级转诊中心接受NACRT及手术切除的直肠癌患者。采用甲基化特异性PCR分析治疗前肿瘤活检标本的CIMP状态(高、中或低)。同时采用焦磷酸测序分析 状态。从病例记录和癌症服务数据库中提取临床信息。通过对切除标本进行组织学检查确定的肿瘤退缩评分来衡量放疗反应。分析这些分子特征、对NACRT的反应与肿瘤学预后之间的关系。
共分析了160例患者,中位随访时间为46.4个月。21例(13%)患者表现出高水平的CIMP甲基化(CIMP-H),与CIMP-L相比,这与壁外血管侵犯(EMVI)风险增加显著相关[8/21(38%)对15/99(15%), = 0.028]。CIMP状态与放疗后肿瘤退缩或生存率无关,然而EMVI与不良生存显著相关( < 0.001)。中等CIMP状态与 突变显著相关( = 0.01)。14例(9%)患者达到病理完全缓解(pCR),而116例(73%)患者在新辅助放化疗后无退缩或退缩极小。达到pCR的患者中位生存期为106个月,退缩极小的患者为65.8个月,尽管差异无统计学意义( = 0.26)。对EMVI与其他预后特征之间关系的二元逻辑回归分析显示,EMVI阳性与总体生存不良、晚期“T”分期和CIMP-H相关,但与淋巴结状态、年龄、性别、 突变状态以及局部或全身复发的存在无关。
我们报告了CIMP-H的治疗前特征与EMVI状态之间的一种新关联,这具有预后意义,且在治疗前组织学检查中不易检测到。