Le Vi T, Klebanoff Mark A, Talavera Maria M, Slaughter Jonathan L
Center for Perinatal Research, The Research Institute at Nationwide Children's Hospital, Columbus, OH, United States of America.
Department of Pediatrics, The Ohio State University, Columbus, OH, United States of America.
PLoS One. 2017 Jun 20;12(6):e0179724. doi: 10.1371/journal.pone.0179724. eCollection 2017.
To evaluate the short-term effects of feed fortification, feed volume increase, and PRBC transfusion on the odds of developing NEC.
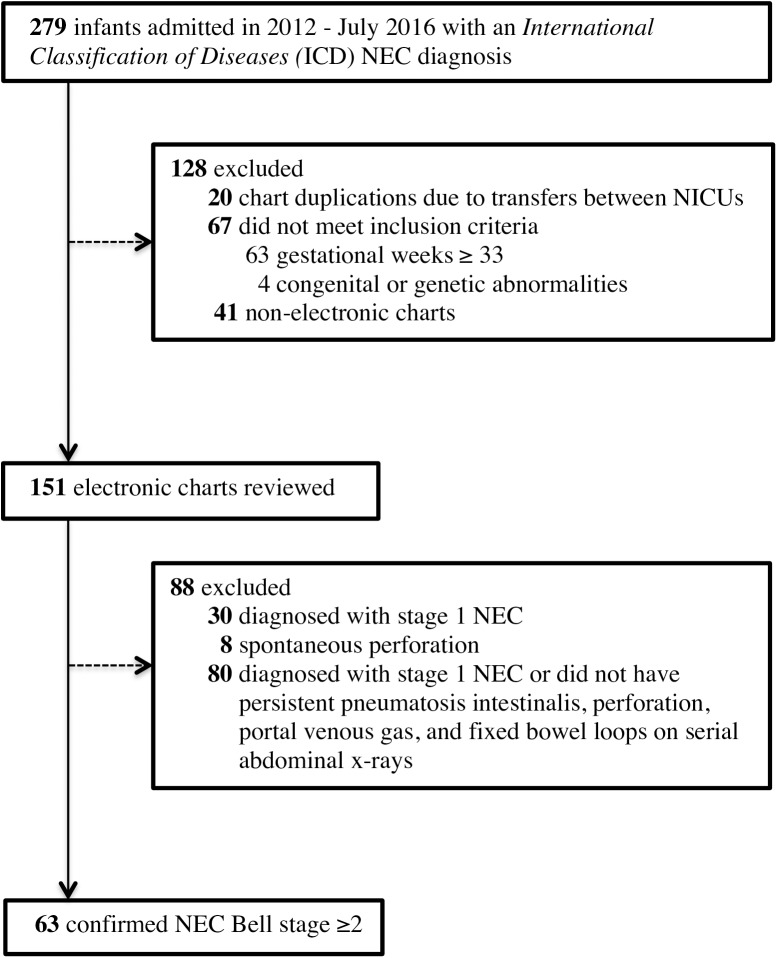
Case-crossover study of neonatal intensive care infants born at ≤ 32 weeks' gestation who were admitted to 5 central Ohio intensive care units from January 2012-July 2016 and developed NEC Bell Stage ≥2. Each patient served as their own control, with exposure during the 48-hour period just prior to NEC onset (hazard period) being compared to a preceding 48-hour control period, thus eliminating confounding by patient factors fixed between both intervals. NEC onset was determined by chart review as the earliest occurrence of one of the following within 24 hours of confirmatory x-ray: (1) antibiotic initiation, (2) enteral feeding cessation, (3) physician first notified of abdominal concerns, or (4) abdominal x-ray ordered. Conditional logistic regression compared exposures to feed volume increase, fortification, and PRBC transfusion during the 48-hour period prior to NEC onset to those during a preceding 48-hour control period. Analyses were stratified by gestational age and anemia (defined: hemoglobin ≤ 9.3 g/dL within 7 days of NEC onset).
We included 63 infants with confirmed NEC. Acute exposure to fortification (odds ratio [OR]: 1.67, 95% confidence interval [CI]: 0.61, 4.59), feed volume increase (OR: 0.63, 95% CI: 0.28, 1.38), and PRBC transfusion (OR: 1.80, 95% CI: 0.60, 5.37) was not associated with the onset of NEC. Gestational age and anemia did not significantly modify the associations. Sensitivity testing substituting 24- and 72-hour hazard and control periods produced similar results.
Using a case-crossover design, we did not detect an association between NEC development and feed fortification, feed volume increase, or PRBC transfusion within 48-hours prior to NEC-onset. Replication in a larger set of cases is needed.
评估强化喂养、增加喂养量和输注浓缩红细胞对坏死性小肠结肠炎(NEC)发病几率的短期影响。
对2012年1月至2016年7月期间入住俄亥俄州中部5家重症监护病房、孕周≤32周且发生NEC Bell分期≥2期的新生儿重症监护患儿进行病例交叉研究。每位患者均作为自身对照,将NEC发病前48小时(危险期)的暴露情况与之前的48小时对照期进行比较,从而消除两个时间段之间固定的患者因素造成的混杂影响。通过病历审查确定NEC发病为确诊X线检查后24小时内最早出现以下情况之一:(1)开始使用抗生素;(2)停止肠内喂养;(3)医生首次接到腹部问题通知;或(4)开具腹部X线检查医嘱。采用条件逻辑回归比较NEC发病前48小时内强化喂养、增加喂养量和输注浓缩红细胞的暴露情况与之前48小时对照期的暴露情况。分析按孕周和贫血情况(定义:NEC发病7天内血红蛋白≤9.3 g/dL)进行分层。
我们纳入了63例确诊为NEC的婴儿。强化喂养(优势比[OR]:1.67,95%置信区间[CI]:0.61,4.59)、增加喂养量(OR:0.63,95% CI:0.28,1.38)和输注浓缩红细胞(OR:1.80,95% CI:0.60,5.37)的急性暴露与NEC发病无关。孕周和贫血情况并未显著改变这些关联。将危险期和对照期分别替换为24小时和72小时进行敏感性测试,结果相似。
采用病例交叉设计,我们未发现NEC发病与NEC发病前48小时内的强化喂养、增加喂养量或输注浓缩红细胞之间存在关联。需要在更大规模的病例中进行重复研究。