Halmagyi G M, Chen Luke, MacDougall Hamish G, Weber Konrad P, McGarvie Leigh A, Curthoys Ian S
Neurology Department, Institute of Clinical Neurosciences, Royal Prince Alfred Hospital, Camperdown, NSW, Australia.
Vestibular Research Laboratory, School of Psychology, The University of Sydney, Sydney, NSW, Australia.
Front Neurol. 2017 Jun 9;8:258. doi: 10.3389/fneur.2017.00258. eCollection 2017.
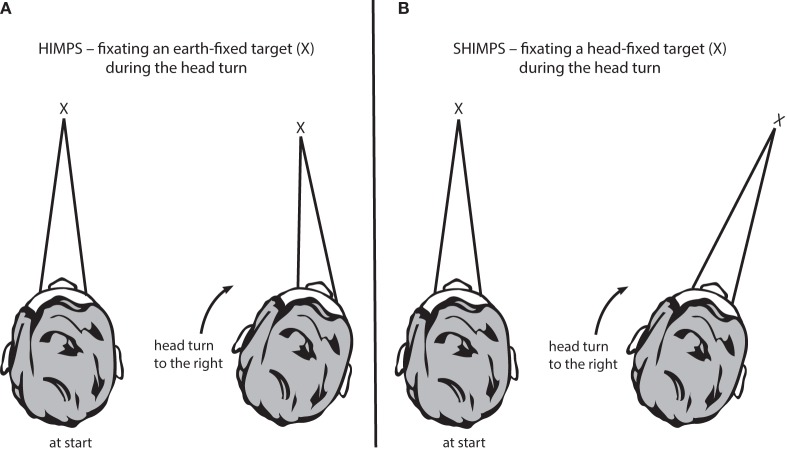
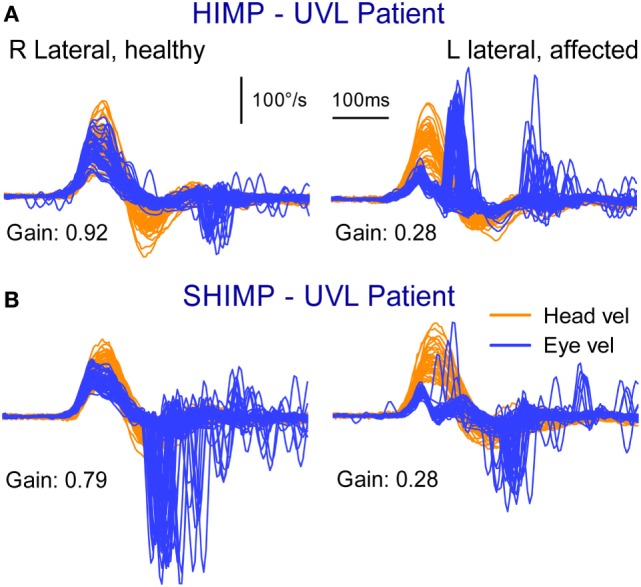
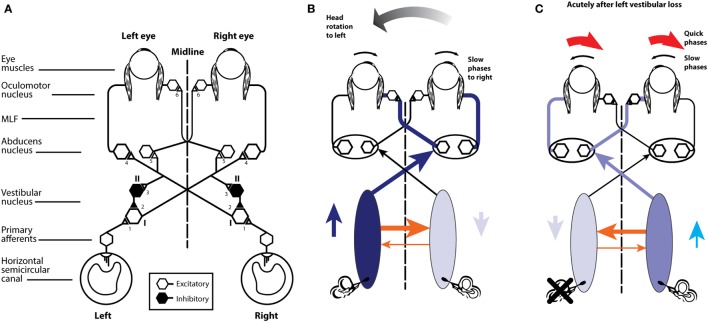
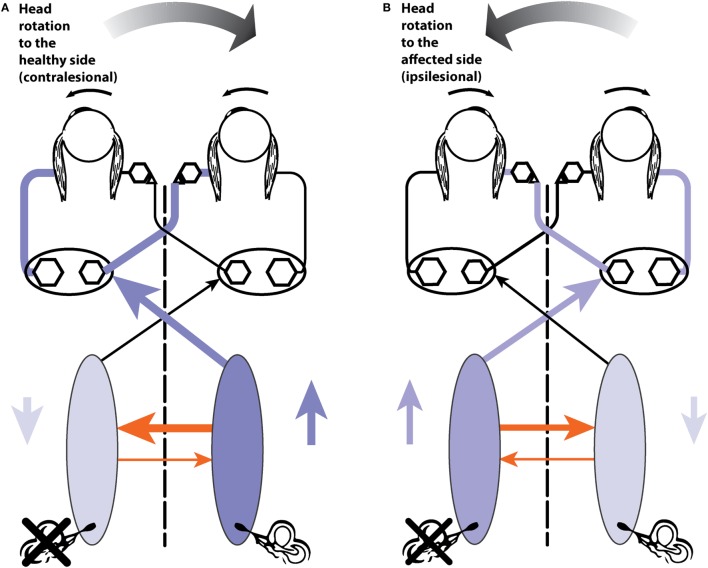
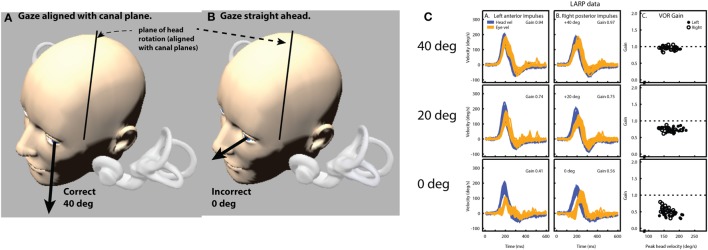
In 1988, we introduced impulsive testing of semicircular canal (SCC) function measured with scleral search coils and showed that it could accurately and reliably detect impaired function even of a single lateral canal. Later we showed that it was also possible to test individual vertical canal function in peripheral and also in central vestibular disorders and proposed a physiological mechanism for why this might be so. For the next 20 years, between 1988 and 2008, impulsive testing of individual SCC function could only be accurately done by a few aficionados with the time and money to support scleral search-coil systems-an expensive, complicated and cumbersome, semi-invasive technique that never made the transition from the research lab to the dizzy clinic. Then, in 2009 and 2013, we introduced a video method of testing function of each of the six canals individually. Since 2009, the method has been taken up by most dizzy clinics around the world, with now close to 100 refereed articles in PubMed. In many dizzy clinics around the world, video Head Impulse Testing has supplanted caloric testing as the initial and in some cases the final test of choice in patients with suspected vestibular disorders. Here, we consider seven current, interesting, and controversial aspects of video Head Impulse Testing: (1) introduction to the test; (2) the progress from the head impulse protocol (HIMPs) to the new variant-suppression head impulse protocol (SHIMPs); (3) the physiological basis for head impulse testing; (4) practical aspects and potential pitfalls of video head impulse testing; (5) problems of vestibulo-ocular reflex gain calculations; (6) head impulse testing in central vestibular disorders; and (7) to stay right up-to-date-new clinical disease patterns emerging from video head impulse testing. With thanks and appreciation we dedicate this article to our friend, colleague, and mentor, Dr Bernard Cohen of Mount Sinai Medical School, New York, who since his first article 55 years ago on compensatory eye movements induced by vertical SCC stimulation has become one of the giants of the vestibular world.
1988年,我们引入了用巩膜搜索线圈测量半规管(SCC)功能的冲动测试,并表明其能够准确可靠地检测出即使是单个外侧半规管的功能受损情况。后来我们又表明,在周围性和中枢性前庭疾病中测试单个垂直半规管功能也是可行的,并提出了其背后可能的生理机制。在接下来的20年里,即1988年至2008年期间,只有少数有时间和资金支持巩膜搜索线圈系统的爱好者才能准确地进行单个SCC功能的冲动测试——这是一种昂贵、复杂且繁琐的半侵入性技术,从未从研究实验室过渡到眩晕门诊。然后,在2009年和2013年,我们推出了一种分别测试六条半规管中每条半规管功能的视频方法。自2009年以来,这种方法已被全球大多数眩晕门诊采用,目前在PubMed上有近100篇经过同行评审的文章。在世界各地的许多眩晕门诊中,视频头脉冲测试已经取代冷热试验,成为疑似前庭疾病患者的初始测试,在某些情况下甚至是最终测试选择。在此,我们探讨视频头脉冲测试当前七个有趣且有争议的方面:(1)测试介绍;(2)从头脉冲方案(HIMPs)到新的变体——抑制性头脉冲方案(SHIMPs)的进展;(3)头脉冲测试的生理基础;(4)视频头脉冲测试的实际操作及潜在陷阱;(5)前庭眼反射增益计算的问题;(6)中枢性前庭疾病中的头脉冲测试;(7)紧跟最新情况——视频头脉冲测试中出现的新临床疾病模式。我们怀着感激之情将本文献给我们的朋友、同事和导师,纽约西奈山医学院的伯纳德·科恩博士,自55年前他发表第一篇关于垂直半规管刺激诱发的代偿性眼动的文章以来,他已成为前庭领域的巨擘之一。