Nordström Carl-Henrik, Koskinen Lars-Owe, Olivecrona Magnus
Department of Neurosurgery, Odense University Hospital, Odense, Denmark.
Department of Clinical Neuroscience, Division of Neurosurgery, Umeå University, Umeå, Sweden.
Front Neurol. 2017 Jun 19;8:274. doi: 10.3389/fneur.2017.00274. eCollection 2017.
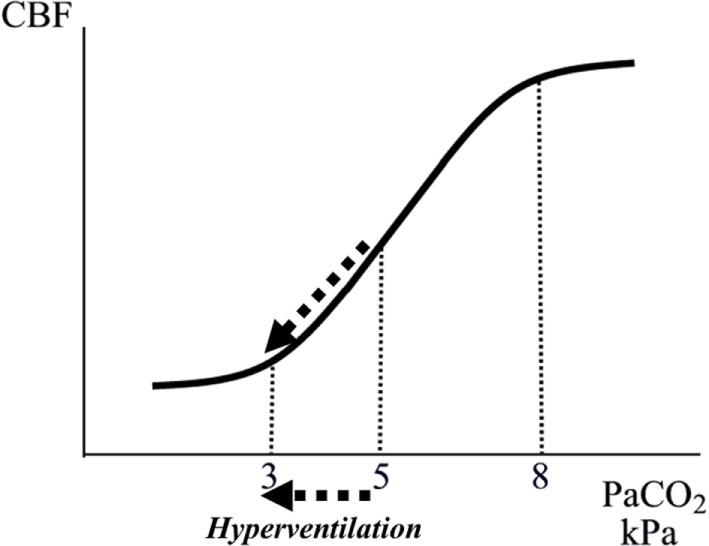
Neurocritical care (NCC) is a branch of intensive care medicine characterized by specific physiological and biochemical monitoring techniques necessary for identifying cerebral adverse events and for evaluating specific therapies. Information is primarily obtained from physiological variables related to intracranial pressure (ICP) and cerebral blood flow (CBF) and from physiological and biochemical variables related to cerebral energy metabolism. Non-surgical therapies developed for treating increased ICP are based on knowledge regarding transport of water across the intact and injured blood-brain barrier (BBB) and the regulation of CBF. Brain volume is strictly controlled as the BBB permeability to crystalloids is very low restricting net transport of water across the capillary wall. Cerebral pressure autoregulation prevents changes in intracranial blood volume and intracapillary hydrostatic pressure at variations in arterial blood pressure. Information regarding cerebral oxidative metabolism is obtained from measurements of brain tissue oxygen tension (PO) and biochemical data obtained from intracerebral microdialysis. As interstitial lactate/pyruvate (LP) ratio instantaneously reflects shifts in intracellular cytoplasmatic redox state, it is an important indicator of compromised cerebral oxidative metabolism. The combined information obtained from PO, LP ratio, and the pattern of biochemical variables reveals whether impaired oxidative metabolism is due to insufficient perfusion (ischemia) or mitochondrial dysfunction. Intracerebral microdialysis and PO give information from a very small volume of tissue. Accordingly, clinical interpretation of the data must be based on information of the probe location in relation to focal brain damage. Attempts to evaluate global cerebral energy state from microdialysis of intraventricular fluid and from the LP ratio of the draining venous blood have recently been presented. To be of clinical relevance, the information from all monitoring techniques should be presented bedside online. Accordingly, in the future, the chemical variables obtained from microdialysis will probably be analyzed by biochemical sensors.
神经重症监护(NCC)是重症监护医学的一个分支,其特点是采用特定的生理和生化监测技术,这些技术对于识别脑部不良事件以及评估特定治疗方法至关重要。信息主要来自与颅内压(ICP)和脑血流量(CBF)相关的生理变量,以及与脑能量代谢相关的生理和生化变量。为治疗ICP升高而开发的非手术疗法是基于有关水在完整和受损血脑屏障(BBB)中的转运以及CBF调节的知识。由于BBB对晶体的通透性非常低,限制了水在毛细血管壁的净转运,因此脑容量受到严格控制。脑压力自动调节可防止动脉血压变化时颅内血容量和毛细血管内静水压力的改变。有关脑氧化代谢的信息来自脑组织氧张力(PO)的测量以及脑内微透析获得的生化数据。由于间质乳酸/丙酮酸(LP)比值可即时反映细胞内细胞质氧化还原状态的变化,因此它是脑氧化代谢受损的重要指标。从PO、LP比值和生化变量模式获得的综合信息揭示了氧化代谢受损是由于灌注不足(缺血)还是线粒体功能障碍。脑内微透析和PO提供来自非常少量组织的信息。因此,数据的临床解释必须基于探头位置与局灶性脑损伤相关的信息。最近有人尝试通过对脑室内液进行微透析以及对引流静脉血的LP比值来评估整体脑能量状态。为了具有临床相关性,所有监测技术的信息都应在床边在线呈现。因此,未来,从微透析获得的化学变量可能会通过生化传感器进行分析。