Jones Kelly M, Balalla Shivanthi, Theadom Alice, Jackman Gordon, Feigin Valery L
National Institute for Stroke and Applied Neurosciences, School of Public Health & Psychosocial Studies, Faculty of Health and Environmental Studies, Auckland University of Technology, North Shore Campus, AA254, 90 Akoranga Dr, Northcote 0627, Private Bag 92006, Auckland, New Zealand.
Polio New Zealand Inc., New Plymouth, New Zealand.
BMJ Open. 2017 Jul 9;7(7):e015470. doi: 10.1136/bmjopen-2016-015470.
Accurate prevalence figures estimating the number of survivors of poliomyelitis (disease causing acute flaccid paralysis) following poliovirus infection are not available. We aim to undertake a systematic review of all literature concerning the prevalence of survivors of poliomyelitis.
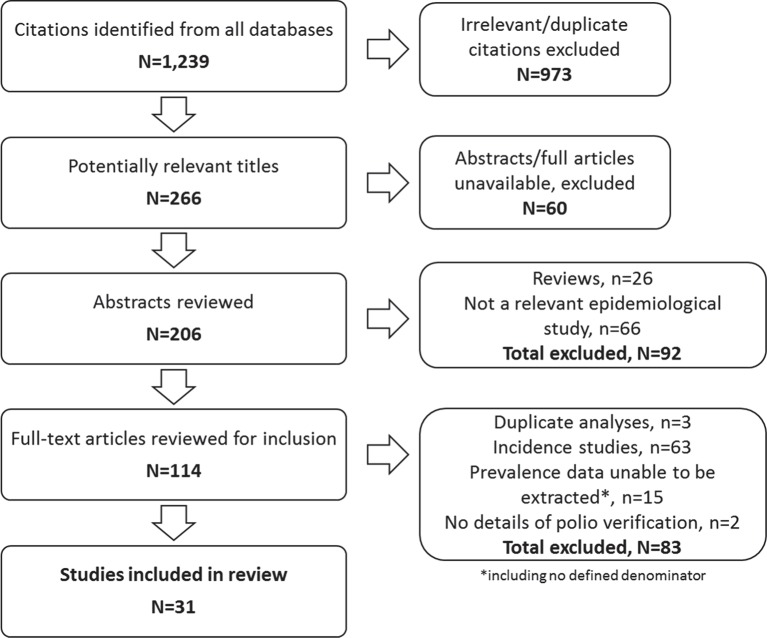
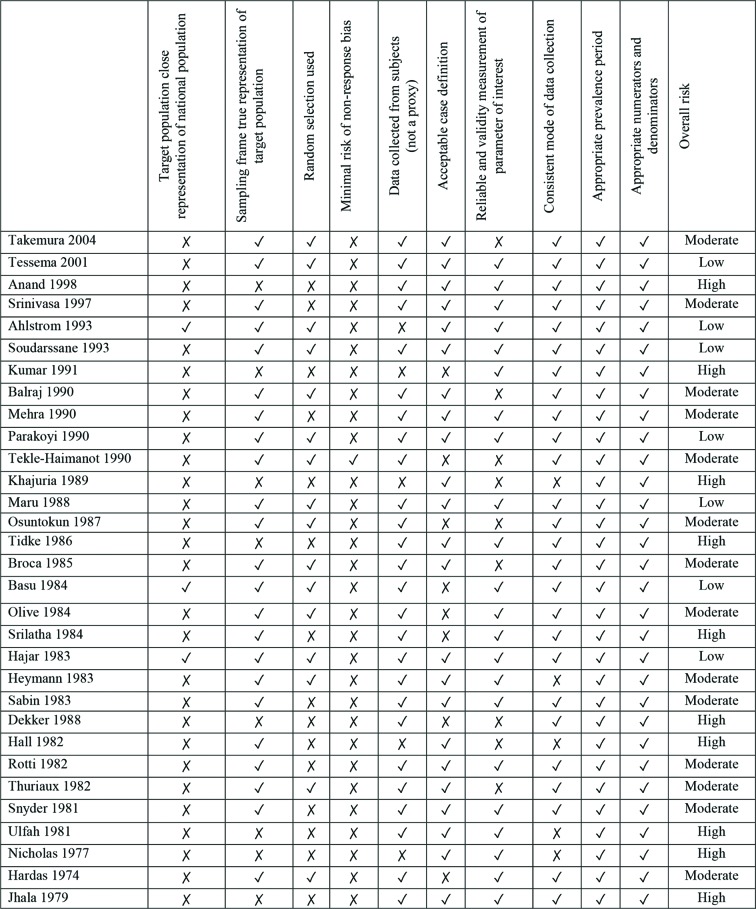
Electronic databases were searched from 1900 up to May 2016 for peer-reviewed studies using a population-based approach witha defined denominator and some form of diagnostic or clinical verification of polio. Exclusion criteria were any prevalence data that were unable to be extracted or calculated and studies reporting on incidence only. The quality of each included study was assessed using an existing tool modified for use in prevalence studies. Average crude prevalence rates were used to calculate worldwide estimates.
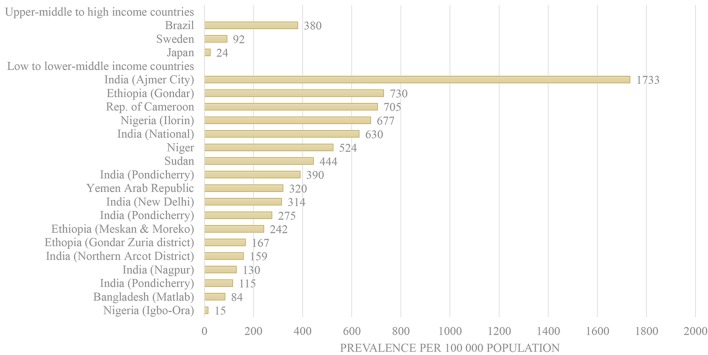
Thirty-one studies met criteria with 90% of studies conducted in low-income to lower middle-income countries. Significant variability in the prevalence of survivors of poliomyelitis was revealed, in low- income to lower middle-income (15 per 100 000 in Nigeria to 1733 in India) and upper-middle to high-income countries (24 (Japan) to 380 per 100 000 (Brazil). The total combined prevalence of survivors of poliomyelitis for those studies at low to moderate risk of bias ranged from 165 (high-income countries) to 425 (low-income to lower middle-income countries) per 100 000 person-years. Historical lameness surveys of children predominated, with wide variation in case definition and assessment criteria, and limited relevance to current prevalence given the lack of incidence of poliovirus infection in the ensuing years.
These results highlight the need for future epidemiological studies of poliomyelitis to examine nationally representative samples, including all ages and greater focus on high-income countries. Such efforts will improve capacity to provide reliable and more robust worldwide prevalence estimates.
目前尚无准确的患病率数据来估计脊髓灰质炎病毒感染后脊髓灰质炎(导致急性弛缓性麻痹的疾病)幸存者的数量。我们旨在对所有关于脊髓灰质炎幸存者患病率的文献进行系统综述。
检索了1900年至2016年5月的电子数据库,以查找采用基于人群的方法、有明确分母且对脊髓灰质炎进行某种形式诊断或临床验证的同行评审研究。排除标准为任何无法提取或计算的患病率数据以及仅报告发病率的研究。使用为患病率研究修改的现有工具评估每项纳入研究的质量。采用平均粗患病率来计算全球估计数。
31项研究符合标准,其中90%的研究在低收入至中低收入国家进行。结果显示,脊髓灰质炎幸存者的患病率存在显著差异,在低收入至中低收入国家(尼日利亚每10万人中有15例至印度每10万人中有1733例)以及中高收入至高收入国家(日本每10万人中有24例至巴西每10万人中有380例)。对于那些偏倚风险低至中等的研究,脊髓灰质炎幸存者的总合并患病率为每10万人年165例(高收入国家)至425例(低收入至中低收入国家)。儿童历史跛行调查占主导,病例定义和评估标准差异很大,且由于随后几年缺乏脊髓灰质炎病毒感染发病率,与当前患病率的相关性有限。
这些结果凸显了未来脊髓灰质炎流行病学研究需要调查具有全国代表性的样本,包括所有年龄段,并更多地关注高收入国家。此类努力将提高提供可靠且更有力的全球患病率估计值的能力。