Peitz Ulrich, Vieth Michael, Evert Matthias, Arand Jovana, Roessner Albert, Malfertheiner Peter
Clinic of Gastroenterology, Hepatology, and Infectious Diseases, Otto-von-Guericke University, Leipziger Str. 44, D 30120, Magdeburg, Germany.
Clinic of Gastroenterology, Raphaelsklinik, Münster, Germany.
BMC Gastroenterol. 2017 Jul 12;17(1):87. doi: 10.1186/s12876-017-0644-3.
The previously reported prevalence of gastric heterotopia in the cervical esophagus, also termed inlet patch (IP), varies substantially, ranging from 0.18 to 14%. Regarding cases with adenocarcinoma within IP, some experts recommend to routinely obtain biopsies from IP for histopathology. Another concern is the reported relation to Barrett's esophagus. The objectives of the study were to prospectively determine the prevalence of IP and of preneoplasia within IP, and to investigate the association between IP and Barrett's esophagus.
372 consecutive patients undergoing esophagogastroduodenoscopy were carefully searched for the presence of IP. Biopsies for histopathology were targeted to the IP, columnar metaplasia of the lower esophagus, gastric corpus and antrum. Different definitions of Barrett's esophagus were tested for an association with IP.
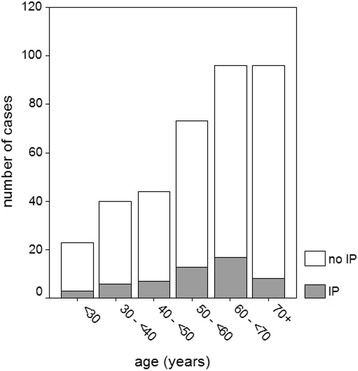
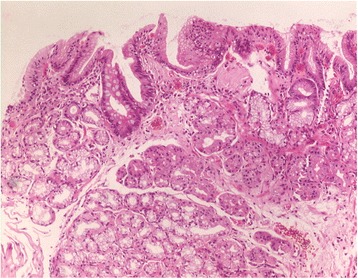
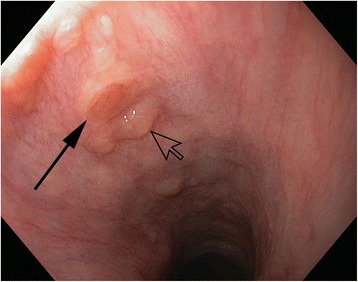
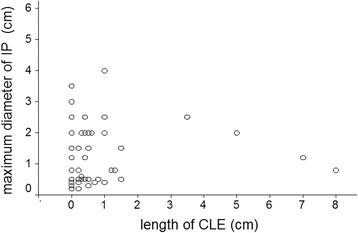
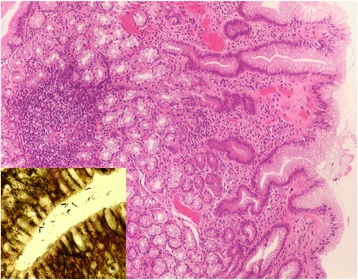
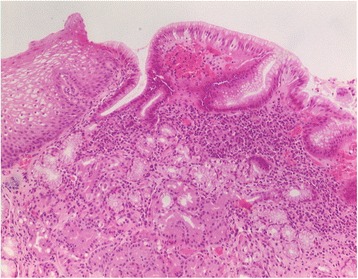
At least one IP was endoscopically identified in 53 patients (14.5%). Histopathology, performed in 46 patients, confirmed columnar epithelium in 87% of cases, which essentially presented corpus and/or cardia-type mucosa. Intestinal metaplasia was detected in two cases, but no neoplasia. A previously reported association of IP with Barrett's esophagus was weak, statistically significant only when short segments of cardia-type mucosa of the lower esophagus were included in the definition of Barrett's esophagus.
The prevalence of IP seems to be underestimated, but preneoplasia within IP is rare, which does not support the recommendation to regularly obtain biopsies for histopathology. Biopsies should be targeted to any irregularities within the heterotopic mucosa. The correlation of IP with Barrett's esophagus hints to a partly common pathogenesis.
先前报道的颈段食管胃异位(也称为入口斑[IP])的患病率差异很大,范围从0.18%至14%。对于IP内发生腺癌的病例,一些专家建议常规获取IP组织进行组织病理学检查。另一个关注点是其与巴雷特食管的报道关系。本研究的目的是前瞻性确定IP的患病率以及IP内的癌前病变,并研究IP与巴雷特食管之间的关联。
对372例连续接受食管胃十二指肠镜检查的患者仔细检查是否存在IP。针对IP、食管下段柱状上皮化生、胃体和胃窦进行组织病理学活检。测试了巴雷特食管的不同定义与IP的关联。
53例患者(14.5%)经内镜检查发现至少一处IP。46例患者进行了组织病理学检查,87%的病例证实为柱状上皮,主要表现为胃体和/或贲门型黏膜。检测到2例肠化生,但无肿瘤形成。先前报道的IP与巴雷特食管的关联较弱,仅当巴雷特食管的定义包括食管下段短段贲门型黏膜时,在统计学上有显著意义。
IP的患病率似乎被低估,但IP内的癌前病变罕见,这不支持常规获取组织进行组织病理学检查的建议。活检应针对异位黏膜内的任何异常。IP与巴雷特食管的相关性提示了部分共同的发病机制。