Araujo Pedro Henrique Xavier Nabuco de, Terra Ricardo Mingarini, Santos Thiago da Silva, Chate Rodrigo Caruso, Paiva Antonio Fernando Lins de, Pêgo-Fernandes Paulo Manuel
. Divisão de Cirurgia Torácica, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
. Divisão de Radiologia, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
J Bras Pneumol. 2017 May-Jun;43(3):190-194. doi: 10.1590/S1806-37562016000000240.
: To evaluate the role of intrapleural positioning of a pleural catheter in early lung expansion and pleurodesis success in patients with recurrent malignant pleural effusion (RMPE).
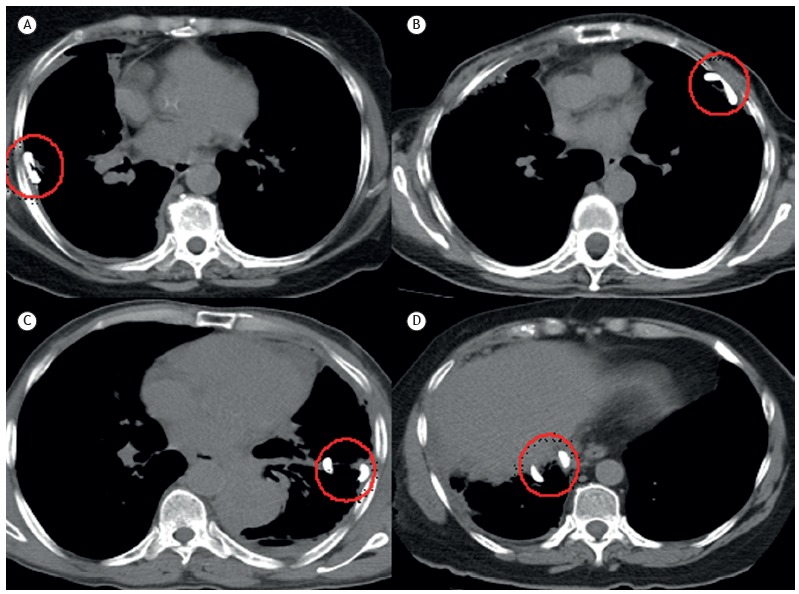
: This was a retrospective study nested into a larger prospective cohort study including patients with RMPE recruited from a tertiary university teaching hospital between June of 2009 and September of 2014. The patients underwent pleural catheter insertion followed by bedside pleurodesis. Chest CT scans were performed twice: immediately before pleurodesis (iCT) and 30 days after pleurodesis (CT30). Catheter positioning was categorized based on iCT scans as posterolateral, anterior, fissural, and subpulmonary. We used the pleural volume on iCT scans to estimate early lung expansion and the difference between the pleural volumes on CT30 and iCT scans to evaluate radiological success of pleurodesis. Clinical pleurodesis success was defined as no need for any other pleural procedure.
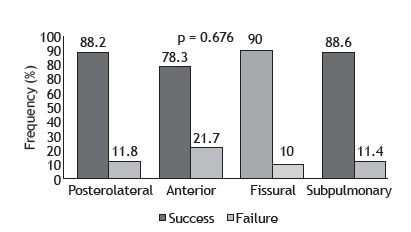
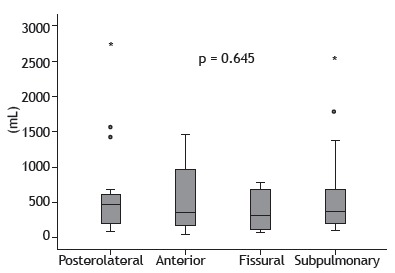
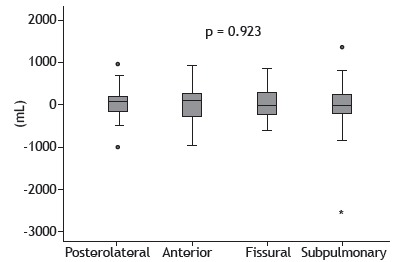
: Of the 131 eligible patients from the original study, 85 were included in this nested study (64 women; mean age: 60.74 years). Catheter tip positioning was subpulmonary in 35 patients (41%), anterior in 23 (27%), posterolateral in 17 (20%), and fissural in 10 (12%). No significant differences were found among the groups regarding early lung expansion (median residual pleural cavity = 377 mL; interquartile range: 171-722 mL; p = 0.645), radiological success of pleurodesis (median volume = 33 mL; interquartile range: -225 to 257 mL; p = 0.923), and clinical success of pleurodesis (85.8%; p = 0.676).
: Our results suggest that the position of the tip of the pleural catheter influences neither early lung expansion nor bedside pleurodesis success in patients with RMPE.
: Avaliar o papel do posicionamento intrapleural do cateter pleural na expansão pulmonar precoce e no sucesso da pleurodese em pacientes com derrame pleural maligno recorrente (DPMR).
MÉTODOS:: Trata-se de um estudo retrospectivo aninhado em um estudo prospectivo de coorte maior com pacientes com DPMR recrutados em um hospital-escola universitário terciário entre junho de 2009 e setembro de 2014. Os pacientes foram submetidos a inserção de cateter pleural e, em seguida, pleurodese à beira do leito. A TC de tórax foi realizada duas vezes: imediatamente antes da pleurodese (TCi) e 30 dias após a pleurodese (TC30). Com base na TCi, a posição do cateter foi classificada em posterolateral, anterior, fissural e subpulmonar. Usamos o volume pleural na TCi para estimar a expansão pulmonar precoce e a diferença entre os volumes pleurais na TC30 e na TCi a fim de avaliar o sucesso radiológico da pleurodese. Considerou-se que a pleurodese teve êxito clínico quando não foi necessário realizar nenhum outro procedimento pleural.
: Dos 131 pacientes elegíveis do estudo original, 85 foram incluídos neste estudo aninhado (64 mulheres; média de idade: 60,74 anos). A posição da ponta do cateter foi subpulmonar em 35 pacientes (41%), anterior em 23 (27%), posterolateral em 17 (20%) e fissural em 10 (12%). Não houve diferenças significativas entre os grupos quanto à expansão pulmonar precoce (mediana da cavidade pleural residual = 377 ml; intervalo interquartil: 171-722 ml; p = 0,645), sucesso radiológico da pleurodese (mediana do volume = 33 ml; intervalo interquartil: -225 a 257 ml; p = 0,923) e sucesso clínico da pleurodese (85,8%; p = 0,676).
CONCLUSÕES:: Nossos resultados sugerem que a posição da ponta do cateter pleural não influencia nem a expansão pulmonar precoce nem o sucesso da pleurodese à beira do leito em pacientes com DPMR.
评估胸膜导管在胸腔内的位置对复发性恶性胸腔积液(RMPE)患者早期肺扩张及胸膜固定术成功率的作用。
这是一项嵌套在大型前瞻性队列研究中的回顾性研究,研究对象为2009年6月至2014年9月从一所三级大学教学医院招募的RMPE患者。患者接受胸膜导管插入术,随后进行床边胸膜固定术。胸部CT扫描进行两次:胸膜固定术前即刻(iCT)和胸膜固定术后30天(CT30)。根据iCT扫描将导管位置分为后外侧、前侧、叶间裂和肺下。我们使用iCT扫描时的胸腔容积来评估早期肺扩张情况,并通过CT30和iCT扫描时胸腔容积的差值来评估胸膜固定术的影像学成功率。临床胸膜固定术成功定义为无需进行任何其他胸膜操作。
在原研究的131例符合条件的患者中,85例纳入了这项嵌套研究(64例女性;平均年龄:60.74岁)。导管尖端位置为肺下的患者有35例(41%),前侧的有23例(27%),后外侧的有17例(20%),叶间裂的有10例(12%)。各组在早期肺扩张(中位残余胸腔 = 377 mL;四分位间距:171 - 722 mL;p = 0.645)、胸膜固定术的影像学成功率(中位容积 = 33 mL;四分位间距:-225至257 mL;p = 0.923)和胸膜固定术的临床成功率(85.8%;p = 0.676)方面均未发现显著差异。
我们的结果表明,胸膜导管尖端的位置对RMPE患者的早期肺扩张及床边胸膜固定术的成功率均无影响。
评估胸膜导管在胸腔内的位置对复发性恶性胸腔积液(DPMR)患者早期肺扩张及胸膜固定术成功率的作用。
这是一项嵌套在大型前瞻性队列研究中的回顾性研究,研究对象为2009年6月至2014年9月从一所三级大学教学医院招募的DPMR患者。患者接受胸膜导管插入术,随后进行床边胸膜固定术。胸部CT扫描进行两次:胸膜固定术前即刻(TCi)和胸膜固定术后30天(TC30)。根据TCi将导管位置分为后外侧、前侧、叶间裂和肺下。我们使用TCi时的胸腔容积来评估早期肺扩张情况,并通过TC30和TCi时胸腔容积的差值来评估胸膜固定术的影像学成功率。当无需进行任何其他胸膜操作时,则认为胸膜固定术临床成功。
在原研究的131例符合条件的患者中,85例纳入了这项嵌套研究(64例女性;平均年龄:60.74岁)。导管尖端位置为肺下的患者有35例(41%),前侧的有23例(27%),后外侧的有17例(20%),叶间裂的有10例(12%)。各组在早期肺扩张(中位残余胸腔 = 377 mL;四分位间距:171 - 722 mL;p = 0.645)、胸膜固定术的影像学成功率(中位容积 = 33 mL;四分位间距:-225至257 mL;p = 0.923)和胸膜固定术的临床成功率(85.8%;p = 0.676)方面均未发现显著差异。
我们的结果表明,胸膜导管尖端的位置对DPMR患者的早期肺扩张及床边胸膜固定术的成功率均无影响。