Li Wenyuan, Dorans Kirsten S, Wilker Elissa H, Rice Mary B, Ljungman Petter L, Schwartz Joel D, Coull Brent A, Koutrakis Petros, Gold Diane R, Keaney John F, Vasan Ramachandran S, Benjamin Emelia J, Mittleman Murray A
From the Departments of Epidemiology (W.L., K.S.D., E.H.W., J.D.S., M.A.M.), Environmental Health (J.D.S., P.K., D.R.G.), and Biostatistics (B.A.C.), Harvard T.H. Chan School of Public Health, Boston, MA; Cardiovascular Epidemiology Research Unit, Division of Cardiology (W.L., K.S.D., E.H.W., P.L.L., M.A.M.) and Division of Pulmonary, Critical Care and Sleep Medicine (M.B.R.), Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA; Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden (P.L.L.); Channing Division of Network Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA (D.R.G.); Division of Cardiovascular Medicine, University of Massachusetts Medical School, Worcester (J.F.K.); National Heart, Lung, and Blood Institute's and Boston University's Framingham Heart Study, MA (R.S.V., E.J.B.); Preventive Medicine and Cardiology Sections, Department of Medicine, Boston University School of Medicine, MA (R.S.V., E.J.B.); and Department of Epidemiology, Boston University School of Public Health, MA (R.S.V., E.J.B.).
Arterioscler Thromb Vasc Biol. 2017 Sep;37(9):1793-1800. doi: 10.1161/ATVBAHA.117.309799. Epub 2017 Jul 27.
The objective of this study is to examine associations between short-term exposure to ambient air pollution and circulating biomarkers of systemic inflammation in participants from the Framingham Offspring and Third Generation cohorts in the greater Boston area.
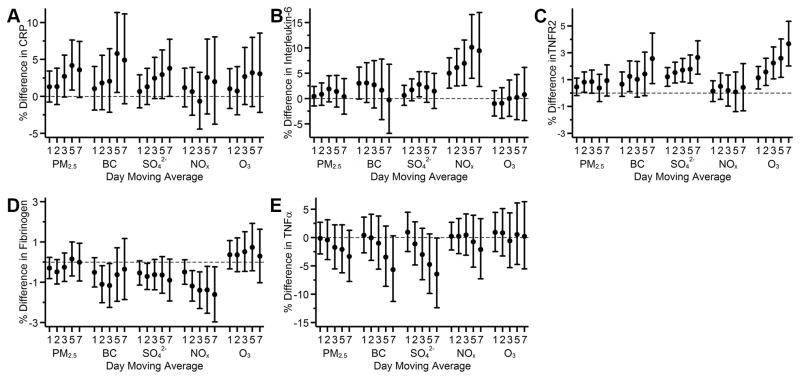
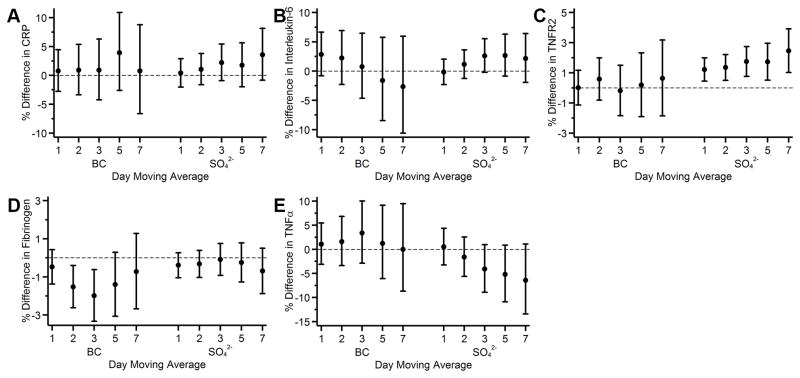
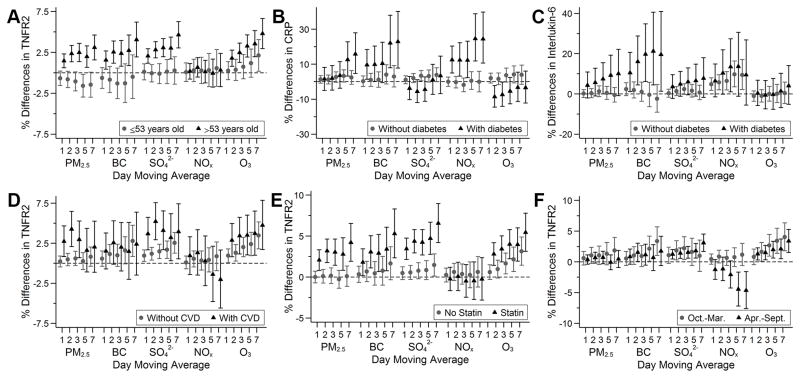
We included 3996 noncurrent smoking participants (mean age, 53.6 years; 54% women) who lived within 50 km from a central air pollution monitoring site in Boston, MA, and calculated the 1- to 7-day moving averages of fine particulate matter (diameter<2.5 µm), black carbon, sulfate, nitrogen oxides, and ozone before the examination visits. We used linear mixed effects models for C-reactive protein and tumor necrosis factor receptor 2, which were measured up to twice for each participant; we used linear regression models for interleukin-6, fibrinogen, and tumor necrosis factor α, which were measured once. We adjusted for demographics, socioeconomic position, lifestyle, time, and weather. The 3- to 7-day moving averages of fine particulate matter (diameter<2.5 µm) and sulfate were positively associated with C-reactive protein concentrations. A 5 µg/m higher 5-day moving average fine particulate matter (diameter<2.5 µm) was associated with 4.2% (95% confidence interval: 0.8, 7.6) higher circulating C-reactive protein. Positive associations were also observed for nitrogen oxides with interleukin-6 and for black carbon, sulfate, and ozone with tumor necrosis factor receptor 2. However, black carbon, sulfate, and nitrogen oxides were negatively associated with fibrinogen, and sulfate was negatively associated with tumor necrosis factor α.
Higher short-term exposure to relatively low levels of ambient air pollution was associated with higher levels of C-reactive protein, interleukin-6, and tumor necrosis factor receptor 2 but not fibrinogen or tumor necrosis factor α in individuals residing in the greater Boston area.
本研究旨在探讨大波士顿地区弗雷明汉后代队列和第三代队列参与者短期暴露于环境空气污染与全身炎症循环生物标志物之间的关联。
我们纳入了3996名非当前吸烟者(平均年龄53.6岁;54%为女性),他们居住在马萨诸塞州波士顿市中心空气污染监测站点50公里范围内,并在检查访视前计算了细颗粒物(直径<2.5微米)、黑碳、硫酸盐、氮氧化物和臭氧的1至7天移动平均值。我们对每个参与者最多测量两次的C反应蛋白和肿瘤坏死因子受体2使用线性混合效应模型;对仅测量一次的白细胞介素-6、纤维蛋白原和肿瘤坏死因子α使用线性回归模型。我们对人口统计学、社会经济地位、生活方式、时间和天气进行了调整。细颗粒物(直径<2.5微米)和硫酸盐的3至7天移动平均值与C反应蛋白浓度呈正相关。5天移动平均细颗粒物(直径<2.5微米)每升高5微克/立方米,循环C反应蛋白升高4.2%(95%置信区间:0.8,7.6)。氮氧化物与白细胞介素-6、黑碳、硫酸盐和臭氧与肿瘤坏死因子受体2之间也观察到正相关。然而,黑碳、硫酸盐和氮氧化物与纤维蛋白原呈负相关,硫酸盐与肿瘤坏死因子α呈负相关。
在大波士顿地区居住的个体中,短期暴露于相对较低水平的环境空气污染与较高水平的C反应蛋白、白细胞介素-6和肿瘤坏死因子受体2相关,但与纤维蛋白原或肿瘤坏死因子α无关。