Department of Biomedical Engineering, Case Western Reserve University, Cleveland, OH, USA.
Department of Urology, James Buchanan Brady Urological Institute, The Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Eur Urol Focus. 2017 Oct;3(4-5):457-466. doi: 10.1016/j.euf.2016.05.009. Epub 2016 Jun 16.
Gleason scoring represents the standard for diagnosis of prostate cancer (PCa) and assessment of prognosis following radical prostatectomy (RP), but it does not account for patterns in neighboring normal-appearing benign fields that may be predictive of disease recurrence.
To investigate (1) whether computer-extracted image features within tumor-adjacent benign regions on digital pathology images could predict recurrence in PCa patients after surgery and (2) whether a tumor plus adjacent benign signature (TABS) could better predict recurrence compared with Gleason score or features from benign or cancerous regions alone.
DESIGN, SETTING, AND PARTICIPANTS: We studied 140 tissue microarray cores (0.6mm each) from 70 PCa patients following surgery between 2000 and 2004 with up to 14 yr of follow-up. Overall, 22 patients experienced recurrence (biochemical [prostate-specific antigen], local, or distant recurrence and cancer death) and 48 did not.
RP was performed in all patients.
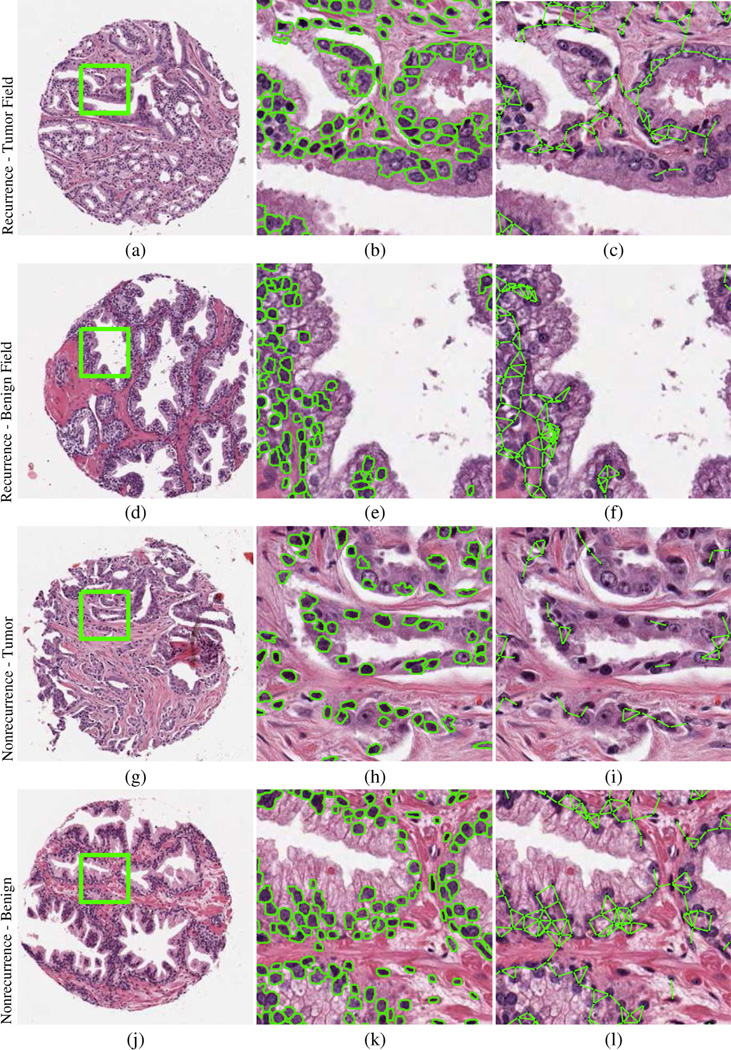
The top 10 features identified as most predictive of recurrence within both the benign and cancerous regions were combined into a 10-feature signature (TABS). Computer-extracted nuclear shape and architectural features from cancerous regions, adjacent benign fields, and TABS were evaluated via random forest classification accuracy and Kaplan-Meier survival analysis.
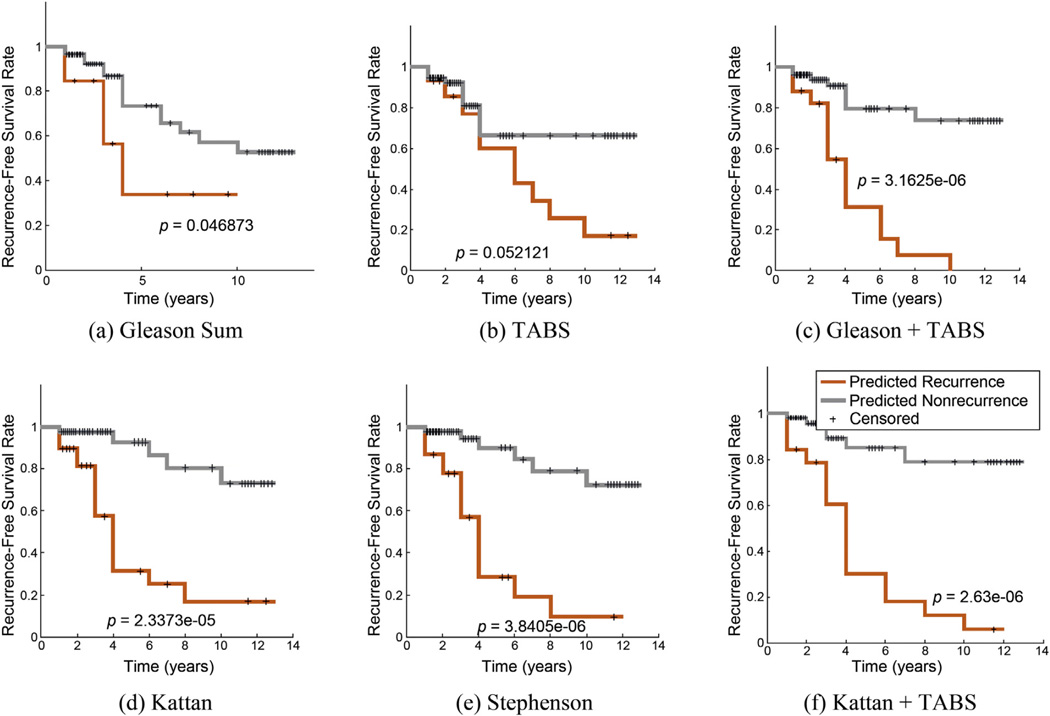
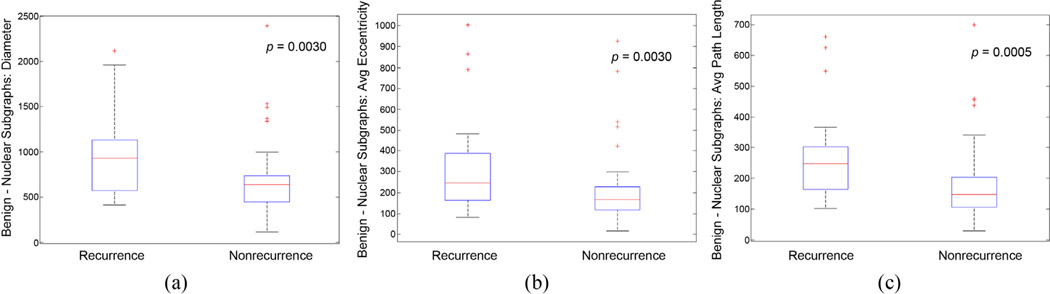
Tumor-adjacent benign field features were predictive of recurrence (area under the receiver operating characteristic curve [AUC]: 0.72). Tumor-field nuclear shape descriptors and benign-field local nuclear arrangement were the predominant features found for TABS (AUC: 0.77). Combining TABS with Gleason sum further improved identification of recurrence (AUC: 0.81). All experiments were performed using threefold cross-validation without independent test set validation.
Computer-extracted nuclear features within cancerous and benign regions predict recurrence following RP. Furthermore, TABS was shown to provide added value to common predictors including Gleason sum and Kattan and Stephenson nomograms.
Future studies may benefit from evaluation of benign regions proximal to the tumor on surgically excised prostate cancer tissue for assessing risk of disease recurrence.
格里森评分是诊断前列腺癌(PCa)和评估根治性前列腺切除术(RP)后预后的标准,但它不能解释肿瘤相邻正常表现的良性区域中的模式,这些模式可能预测疾病复发。
研究(1)在数字病理学图像中肿瘤相邻的良性区域内计算机提取的图像特征是否可以预测手术后 PCa 患者的复发,以及(2)与格里森评分或仅来自良性或癌性区域的特征相比,肿瘤加相邻良性特征(TABS)是否可以更好地预测复发。
设计、地点和参与者:我们研究了 2000 年至 2004 年期间接受手术的 70 例 PCa 患者的 140 个组织微阵列核心(每个 0.6mm),随访时间长达 14 年。总体而言,22 例患者发生复发(生化[前列腺特异性抗原]、局部或远处复发和癌症死亡),48 例未复发。
所有患者均行 RP。
在良性和癌性区域内被确定为最能预测复发的前 10 个特征被组合成一个 10 特征特征(TABS)。通过随机森林分类准确性和 Kaplan-Meier 生存分析评估从癌性区域、相邻良性区域和 TABS 中计算机提取的核形状和结构特征。
肿瘤相邻的良性区域特征可预测复发(接收者操作特征曲线下面积[AUC]:0.72)。肿瘤区域核形状描述符和良性区域局部核排列是 TABS 的主要特征(AUC:0.77)。将 TABS 与格里森总和结合使用可进一步提高对复发的识别能力(AUC:0.81)。所有实验均使用三折交叉验证进行,而无需独立测试集验证。
癌性和良性区域内计算机提取的核特征可预测 RP 后的复发。此外,TABS 被证明可为包括格里森总和、卡坦和斯蒂芬森列线图在内的常见预测因子提供附加价值。
未来的研究可能受益于评估手术切除的前列腺癌组织中肿瘤近端的良性区域,以评估疾病复发的风险。