He Chao, Wang Bo, Li Danni, Xu Huan, Shen Yongchun
Department of Laboratory Medicine Intensive Care Unit Department of Respiratory and Critical Care Medicine, West China Hospital of Sichuan University, Chengdu, Sichuan Province, China.
Medicine (Baltimore). 2017 Aug;96(33):e7829. doi: 10.1097/MD.0000000000007829.
Parapneumonic pleural effusion (PPE) is a common complication of pneumonia. The accurate diagnosis of PPE remains a challenge. Recent studies suggest that procalcitonin (PCT) emerges as a potential biomarker for PPE. Our study aimed to determine the diagnostic value of PCT for PPE by a clinical study and summarize the overall diagnostic performance of PCT through a meta-analysis.
Demographic and clinical data of the patients with PPE and controls were collected in our clinical study. The diagnostic performances of serum PCT (s-PCT) were analyzed via receiver operating characteristic (ROC) curve analysis, using area under the curve (AUC) as a measure of accuracy. Literature databases were systematically searched for the studies examining the accuracy of PCT for diagnosing PPE. Data on sensitivity, specificity, positive/negative likelihood ratio (PLR/NLR), and diagnostic odds ratio (DOR) were pooled. Summary ROC curves and AUC were used to evaluate overall test performance.
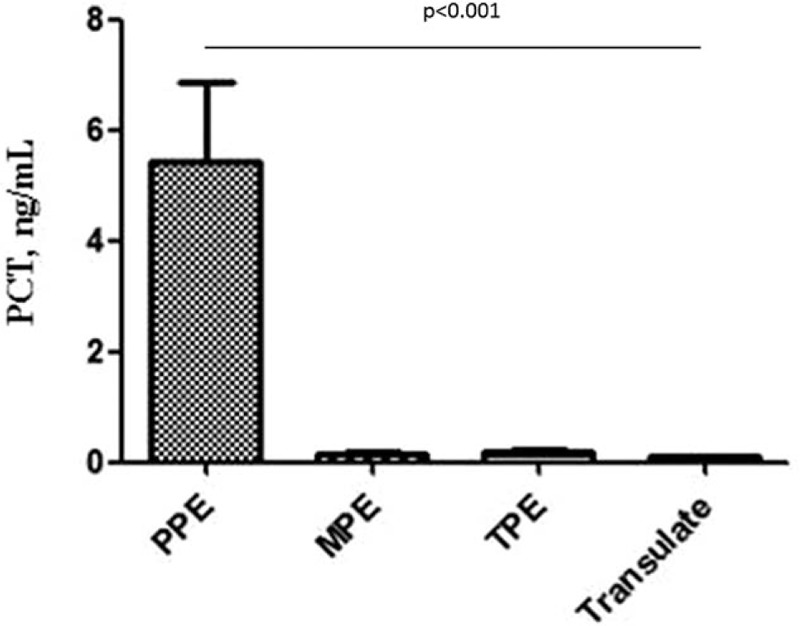
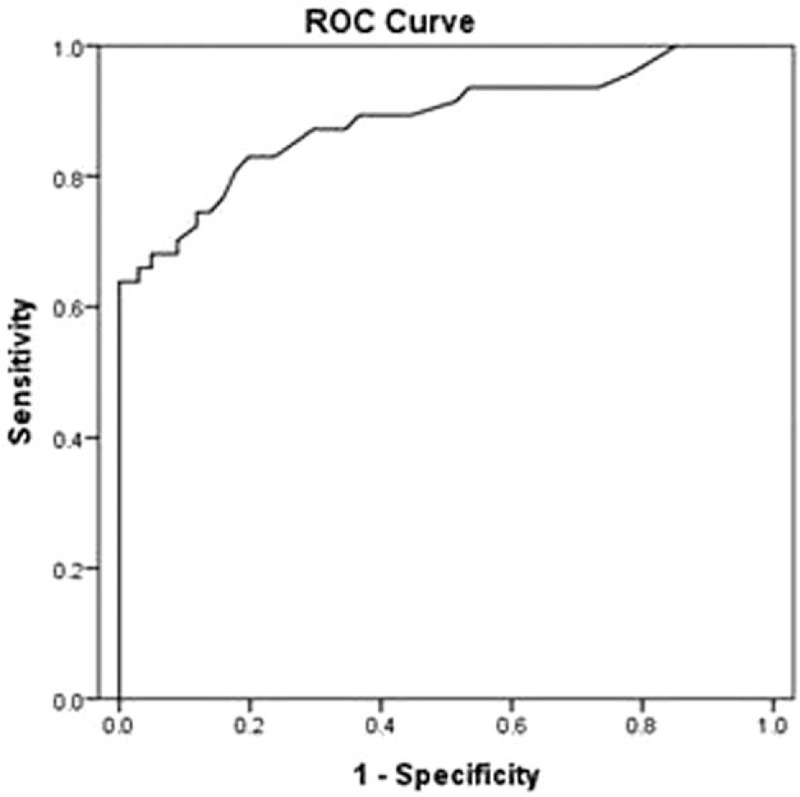
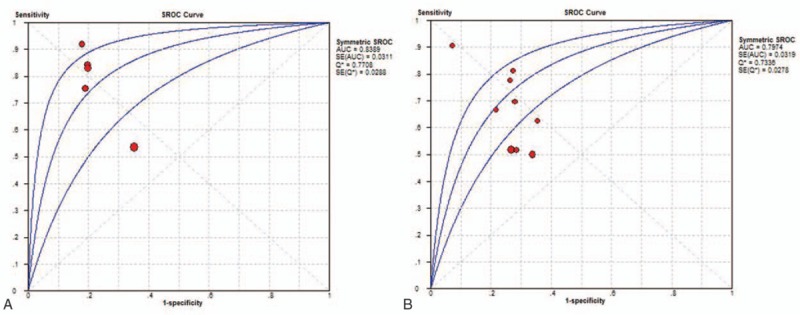
In our clinical study, 47 patients with PPE and 101 controls were included. The s-PCT levels were significantly increased in the setting of PPE (5.44 ± 9.82 ng/mL) compared with malignant PE (0.15 ± 0.19 ng/mL), tuberculous PE (0.18 ± 0.16 ng/mL), and transudates (0.09 ± 0.03 ng/mL) (P < .001). Using a cutoff value of 0.195 ng/mL, the sensitivity and specificity of s-PCT in diagnosing PPE were 0.83 and 0.80, respectively, and AUC was 0.89. In addition, 11 studies were included in our meta-analysis. Summary performance estimates for s-PCT in diagnosing PPE were as follows: sensitivity, 0.78 (95% CI: 0.71-0.84); specificity, 0.74 (95% CI: 0.69-0.78); PLR, 3.46 (95% CI: 2.09-5.74); NLR, 0.27 (95% CI: 0.14-0.54); DOR, 12.37 (95% CI: 4.34-41.17); and AUC, 0.84. The corresponding estimates for p-PCT were as follows: sensitivity, 0.62 (95% CI: 0.57-0.67); specificity, 0.71 (95% CI: 0.68-0.75); PLR 2.31 (95% CI: 1.81-2.95); NLR, 0.47 (95% CI: 0.35-0.63); DOR, 5.48 (95% CI: 3.07-9.77); and AUC, 0.80.
Both s-PCT and p-PCT might have modest performance in diagnosing PPE. However, more studies on a large scale should be performed to confirm our findings.
肺炎旁胸腔积液(PPE)是肺炎的常见并发症。PPE的准确诊断仍然是一项挑战。最近的研究表明,降钙素原(PCT)成为PPE的一种潜在生物标志物。我们的研究旨在通过临床研究确定PCT对PPE的诊断价值,并通过荟萃分析总结PCT的总体诊断性能。
在我们的临床研究中收集了PPE患者和对照组的人口统计学和临床数据。通过受试者工作特征(ROC)曲线分析来分析血清PCT(s-PCT)的诊断性能,使用曲线下面积(AUC)作为准确性的衡量指标。系统检索文献数据库以查找检验PCT诊断PPE准确性的研究。汇总敏感性、特异性、阳性/阴性似然比(PLR/NLR)和诊断比值比(DOR)的数据。使用汇总ROC曲线和AUC来评估总体检验性能。
在我们的临床研究中,纳入了47例PPE患者和101例对照。与恶性胸腔积液(0.15±0.19 ng/mL)、结核性胸腔积液(0.18±0.16 ng/mL)和漏出液(0.09±0.03 ng/mL)相比,PPE患者的s-PCT水平显著升高(5.44±9.82 ng/mL)(P<0.001)。使用0.195 ng/mL的截断值,s-PCT诊断PPE的敏感性和特异性分别为0.83和0.80,AUC为0.89。此外,我们的荟萃分析纳入了11项研究。s-PCT诊断PPE的汇总性能估计如下:敏感性为0.78(95%CI:0.71-0.84);特异性为0.74(95%CI:0.69-0.78);PLR为3.46(95%CI:2.09-5.74);NLR为0.27(95%CI:0.14-0.54);DOR为12.37(95%CI:4.34-41.17);AUC为0.84。p-PCT的相应估计如下:敏感性为0.62(95%CI:0.57-0.67);特异性为0.71(95%CI:0.68-0.75);PLR为2.31(95%CI:1.81-2.95);NLR为0.47(95%CI:0.35-0.63);DOR为5.48(95%CI:3.07-9.77);AUC为0.80。
s-PCT和p-PCT在诊断PPE方面可能都有一定表现。然而,需要进行更多大规模研究来证实我们的发现。