Department of General Surgery, İstanbul University İstanbul School of Medicine, İstanbul, Turkey.
Department of General Surgery, Koç University School of Medicine, İstanbul, Turkey.
Balkan Med J. 2018 Jan 20;35(1):36-42. doi: 10.4274/balkanmedj.2017.0161. Epub 2017 Aug 25.
A thyroidectomy can be performed via a cervical incision in most patients with retrosternal goiter.
To investigate the correlation between the volume of the mediastinal portion of the thyroid gland and the need for an extra-cervical approach for retrosternal goiter.
Diagnostic accuracy study.
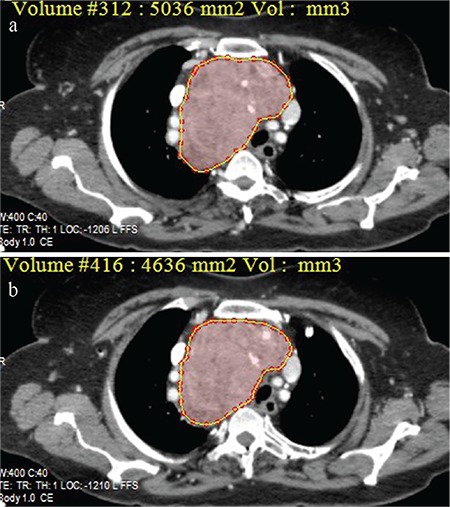
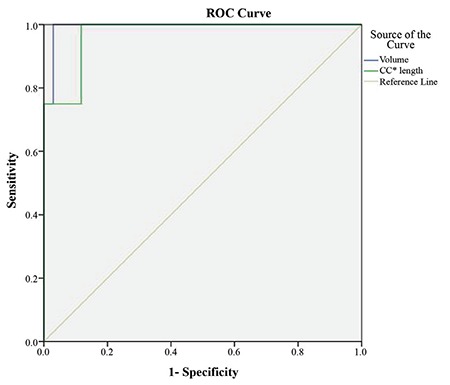
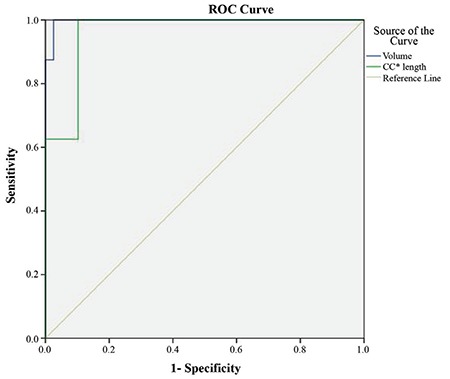
The measurement of craniocaudal length and the volume of the mediastinal component of the thyroid gland on computerised tomography images was performed in 47 patients with retrosternal goiter. Of these 47 patients, 8 (17%) required an extra-cervical approach and were classified as group 1, and 39 (83%) patients that required a cervical incision were classified as group 2. Receiver operating characteristic analysis was performed to determine the cut-off value for the craniocaudal length and the volume of the mediastinal thyroid mass, which significantly correlated with an extra-cervical approach for retrosternal goiter.
Reoperative surgery was significantly more frequent in group 1 than in group 2 (50% vs 13%; p=0.03). The craniocaudal length of the mediastinal thyroid gland was significantly longer in group 1 than in group 2 (77±11 mm vs 31±21 mm, respectively; p=0.0001). The volume of the mediastinal component was significantly larger in group 1 compared to group 2 (264±106 cm3 vs 40±41 cm3, respectively; p=0.0001). The receiver operating characteristic curve of craniocaudal length and the volume of the mediastinal component identified ≥66 mm and ≥162 cm3 as the cut-off values with the maximum accuracy, respectively. The craniocaudal length of the thyroid mass below the thoracic inlet ≥66 mm or a volume of the mediastinal portion ≥162 cm3 were significantly associated with an extra-cervical approach (p=0.0001). For predicting an extra-cervical approach, the sensitivity, positive predictive value and negative predictive value of the cut-off value for craniocaudal length was 87.5%, 64% and 97%, respectively. For predicting an extra-cervical approach, the sensitivity, positive predictive value and negative predictive value of the cut-off values for the mediastinal volume were 100%, 89% and 100%, respectively.
A thyroid volume of ≥162 cm3 extending below the thoracic inlet was a significant determining factor for an extra-cervical approach, with a negative predictive value for the extra-cervical approach of 100% for retrosternal goiter with smaller volumes. Further studies with an increased number of patients are needed to determine the value of volumetric analysis of retrosternal goiter to predict the need for an extra-cervical approach in retrosternal goiter.
大多数胸骨后甲状腺肿患者可通过颈部切口行甲状腺切除术。
探讨胸骨后甲状腺肿纵隔部分体积与颈外入路需求的相关性。
诊断准确性研究。
对 47 例胸骨后甲状腺肿患者的计算机断层扫描图像进行颅尾长度和纵隔甲状腺体积的测量。这 47 例患者中,8 例(17%)需要颈外入路,分为第 1 组,39 例(83%)需要颈部切口,分为第 2 组。进行受试者工作特征分析,以确定颅尾长度和纵隔甲状腺肿块体积的截断值,这些值与胸骨后甲状腺肿的颈外入路显著相关。
第 1 组的再次手术明显比第 2 组更频繁(50%比 13%;p=0.03)。第 1 组的纵隔甲状腺的颅尾长度明显长于第 2 组(77±11mm 比 31±21mm,p=0.0001)。第 1 组的纵隔成分体积明显大于第 2 组(264±106cm3 比 40±41cm3,p=0.0001)。颅尾长度和纵隔成分体积的受试者工作特征曲线分别确定≥66mm 和≥162cm3 为最大准确性的截断值。胸廓入口以下甲状腺肿块的颅尾长度≥66mm 或纵隔部分的体积≥162cm3 与颈外入路显著相关(p=0.0001)。对于预测颈外入路,颅尾长度截断值的敏感性、阳性预测值和阴性预测值分别为 87.5%、64%和 97%。对于预测颈外入路,纵隔体积截断值的敏感性、阳性预测值和阴性预测值分别为 100%、89%和 100%。
延伸至胸廓入口以下的≥162cm3 的甲状腺体积是颈外入路的重要决定因素,对于体积较小的胸骨后甲状腺肿,颈外入路的阴性预测值为 100%。需要进一步的研究来确定胸骨后甲状腺肿体积分析对预测胸骨后甲状腺肿颈外入路需求的价值。