Swiss Tropical and Public Health Institute, Basel, Switzerland.
University of Basel, Basel, Switzerland.
Parasit Vectors. 2017 Sep 30;10(1):450. doi: 10.1186/s13071-017-2393-0.
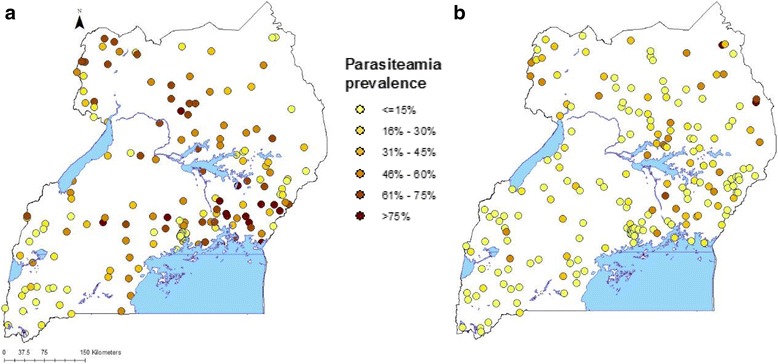
In Uganda, malaria vector control interventions and case management with Artemisinin Combination Therapies (ACTs) have been scaled up over the last few years as a result of increased funding. Data on parasitaemia prevalence among children less than 5 years old and coverage of interventions was collected during the first two Malaria Indicator Surveys (MIS) conducted in 2009 and 2014, respectively. In this study, we quantify the effects of control interventions on parasitaemia risk changes between the two MIS in a spatio-temporal analysis.
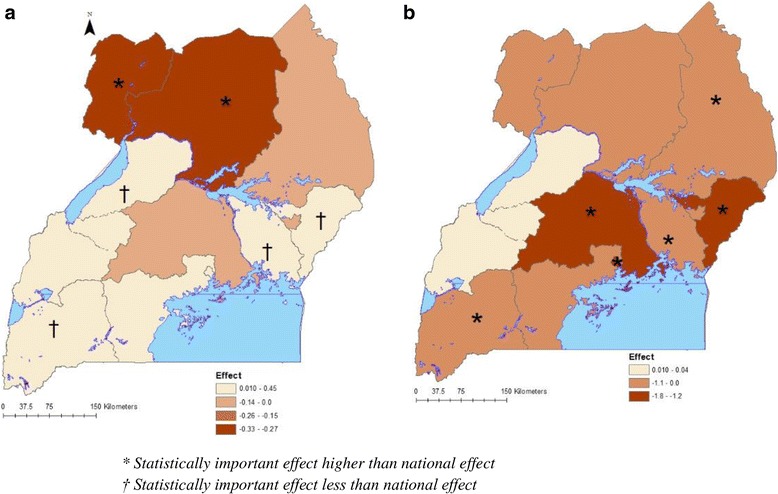
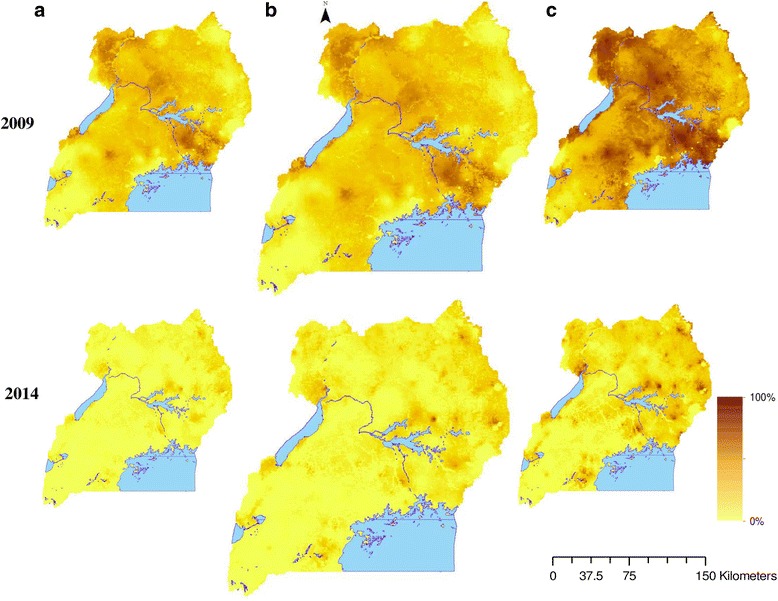
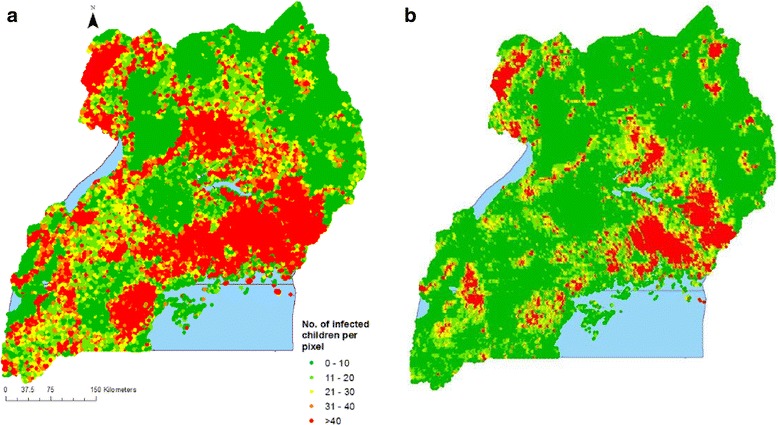
Bayesian geostatistical and temporal models were fitted on the MIS data of 2009 and 2014. The models took into account geographical misalignment in the locations of the two surveys and adjusted for climatic changes and socio-economic differentials. Parasitaemia risk was predicted over a 2 × 2 km grid and the number of infected children less than 5 years old was estimated. Geostatistical variable selection was applied to identify the most important ITN coverage indicators. A spatially varying coefficient model was used to estimate intervention effects at sub-national level.
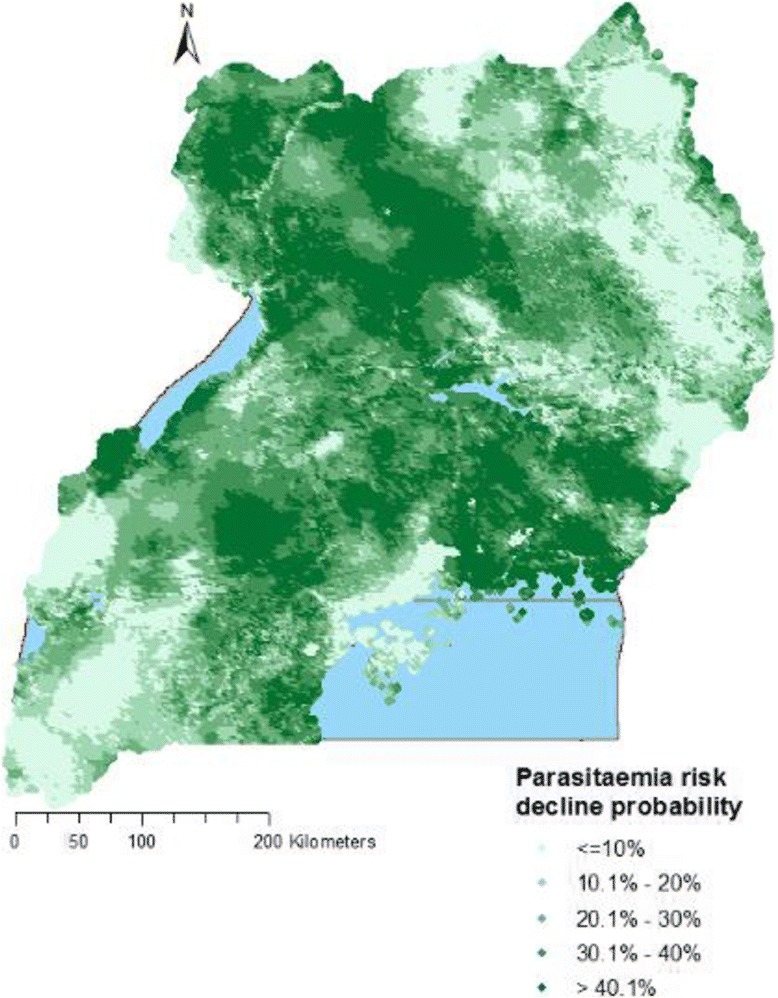
The coverage of Insecticide Treated Nets (ITNs) and ACTs more than doubled at country and sub-national levels during the period 2009-2014. The coverage of Indoor Residual Spraying (IRS) remained static at all levels. ITNs, IRS, and ACTs were associated with a reduction in parasitaemia odds of 19% (95% BCI: 18-29%), 78% (95% BCI: 67-84%), and 34% (95% BCI: 28-66%), respectively. Intervention effects varied with region. Higher socio-economic status and living in urban areas were associated with parasitaemia odds reduction of 46% (95% BCI: 0.51-0.57) and 57% (95% BCI: 0.40-0.53), respectively. The probability of parasitaemia risk decline in the country was 85% and varied from 70% in the North-East region to 100% in Kampala region. The estimated number of children infected with malaria declined from 2,480,373 in 2009 to 825,636 in 2014.
Interventions have had a strong effect on the decline of parasitaemia risk in Uganda during 2009-2014, albeit with varying magnitude in the regions. This success should be sustained by optimizing ITN coverage to achieve universal coverage.
在过去几年中,乌干达由于资金增加,已扩大疟疾媒介控制干预措施和青蒿素联合疗法(ACT)的病例管理。在 2009 年和 2014 年分别进行的前两次疟疾指标调查(MIS)中,收集了 5 岁以下儿童寄生虫血症患病率和干预措施覆盖率的数据。在这项研究中,我们通过时空分析来量化控制干预措施对两次 MIS 之间寄生虫血症风险变化的影响。
对 2009 年和 2014 年 MIS 数据进行贝叶斯地统计学和时间模型拟合。模型考虑了两次调查地点的地理位置不匹配,并调整了气候变化和社会经济差异。在 2×2km 的网格上预测寄生虫血症风险,并估计 5 岁以下受感染儿童的数量。应用地统计学变量选择来确定最重要的 ITN 覆盖率指标。使用空间变化系数模型估计国家以下各级的干预效果。
2009-2014 年期间,全国和国家以下各级的驱虫蚊帐(ITN)和 ACT 覆盖率增加了一倍以上。室内滞留喷洒(IRS)的覆盖率在所有级别均保持不变。ITN、IRS 和 ACT 与寄生虫血症几率降低 19%(95%BCI:18-29%)、78%(95%BCI:67-84%)和 34%(95%BCI:28-66%)相关。干预效果因地区而异。较高的社会经济地位和居住在城市地区与寄生虫血症几率降低 46%(95%BCI:0.51-0.57)和 57%(95%BCI:0.40-0.53)相关。全国寄生虫血症风险下降的概率为 85%,从东北部地区的 70%到坎帕拉地区的 100%不等。估计患有疟疾的儿童人数从 2009 年的 2480373 人减少到 2014 年的 825636 人。
在 2009-2014 年期间,干预措施对乌干达寄生虫血症风险的下降产生了重大影响,但在不同地区的效果不同。通过优化 ITN 覆盖率以实现普遍覆盖,应维持这一成功。