Midwifery Science, AVAG, Amsterdam Public Health research institute, VU University Medical Center, Van der Boechorststraat 7, 1081, BT, Amsterdam, the Netherlands.
Department of Epidemiology and Biostatistics and Amsterdam Public Health research institute, VU University Medical Center, Van der Boechorststraat 7, 1081, BT, Amsterdam, the Netherlands.
BMC Pregnancy Childbirth. 2017 Oct 16;17(1):353. doi: 10.1186/s12884-017-1513-3.
Screening for, diagnosis and management of intrauterine growth restriction (IUGR) is often performed in multidisciplinary collaboration. However, variation in screening methods, diagnosis and management of IUGR may lead to confusion. In the Netherlands two monodisciplinary guidelines on IUGR do not fully align. To facilitate effective collaboration between different professionals in perinatal care, we undertook a Delphi study with uniform recommendations as our primary result, focusing on issues that are not aligned or for which specifications are lacking in the current guidelines.
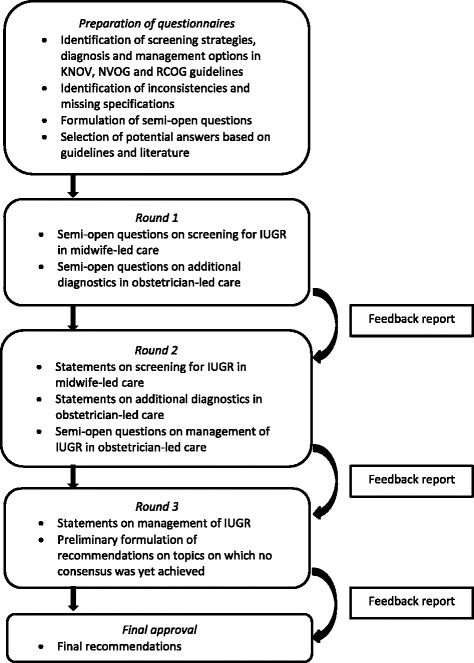
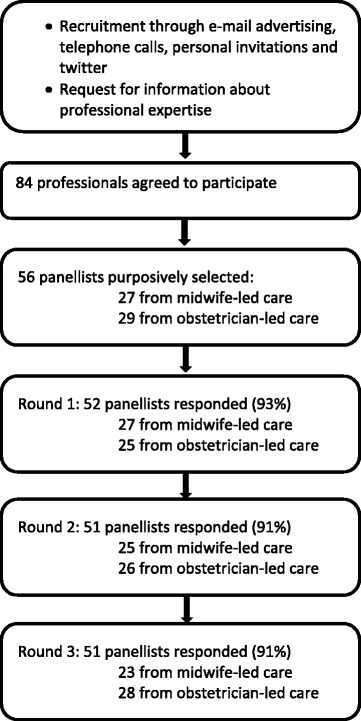
We conducted a Delphi study in three rounds. A purposively sampled selection of 56 panellists participated: 27 representing midwife-led care and 29 obstetrician-led care. Consensus was defined as agreement between the professional groups on the same answer and among at least 70% of the panellists within groups.
Per round 51 or 52 (91% - 93%) panellists responded. This has led to consensus on 27 issues, leading to four consensus based recommendations on screening for IUGR in midwife-led care and eight consensus based recommendations on diagnosis and eight on management in obstetrician-led care. The multidisciplinary project group decided on four additional recommendations as no consensus was reached by the panel. No recommendations could be made about induction of labour versus expectant monitoring, nor about the choice for a primary caesarean section.
We reached consensus on recommendations for care for IUGR within a multidisciplinary panel. These will be implemented in a study on the effectiveness and cost-effectiveness of routine third trimester ultrasound for monitoring fetal growth. Research is needed to evaluate the effects of implementation of these recommendations on perinatal outcomes.
NTR4367 .
宫内生长受限(IUGR)的筛查、诊断和管理通常是多学科合作进行的。然而,筛查方法、IUGR 的诊断和管理的差异可能会导致混淆。在荷兰,两份关于 IUGR 的单学科指南并不完全一致。为了促进围产期护理中不同专业人员之间的有效合作,我们进行了一项德尔菲研究,以统一的建议作为主要结果,重点关注当前指南中不一致或缺乏规范的问题。
我们进行了三轮德尔菲研究。有目的选择了 56 名专家参与:27 名代表助产士主导的护理,29 名代表产科医生主导的护理。共识定义为专业组之间对相同答案的一致意见,以及组内至少 70%的专家的一致意见。
每轮有 51 或 52 名(91%-93%)专家做出回应。这导致了 27 个问题的共识,从而产生了四项关于助产士主导的护理中 IUGR 筛查的共识建议,八项关于产科医生主导的护理中诊断和管理的共识建议。多学科项目组决定增加四项额外建议,因为专家组没有达成共识。对于引产与期待监测、初次剖宫产的选择,无法提出建议。
我们在多学科专家组中就 IUGR 护理的建议达成了共识。这些建议将在一项关于常规孕晚期超声监测胎儿生长的有效性和成本效益的研究中实施。需要研究这些建议的实施对围产结局的影响。
NTR4367。