Office of Biostatistics and Quantitative Health Sciences, John A. Burns School of Medicine, 651 Ilalo St, Biosciences Bldg, 211C, Honolulu, HI 96813. Email:
Department of Pharmacy Practice, Daniel K. Inouye College of Pharmacy at the University of Hawai'i at Hilo, Hilo, Hawai'i.
Prev Chronic Dis. 2017 Oct 19;14:E101. doi: 10.5888/pcd14.160241.
Diabetes, cancer, cardiovascular disease (CVD) (coronary artery disease, heart attack, and angina pectoris), and chronic lung disease (emphysema, chronic bronchitis, and chronic obstructive pulmonary disease) are major causes of death in the United States. The objective of this study was to assess racial/ethnic differences in the prevalence of these conditions as cause of death among people aged 60 to 79 years with one or more of these conditions.
We used data on the prevalence of major chronic conditions from the National Health Interview Survey on 56,290 adults aged 60 to 79 years who reported having any of the chronic conditions assessed in the National Health Interview Survey for 2006 through 2014. We compared trends with age for 11 single and multiple conditions. Analyses employed multinomial logistic regression models.
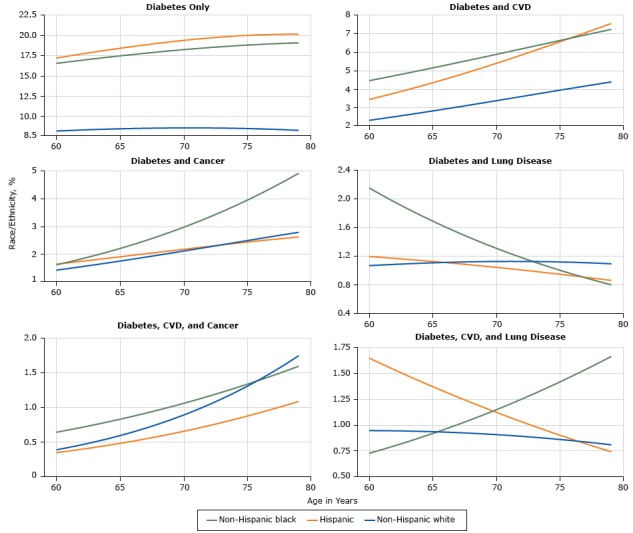
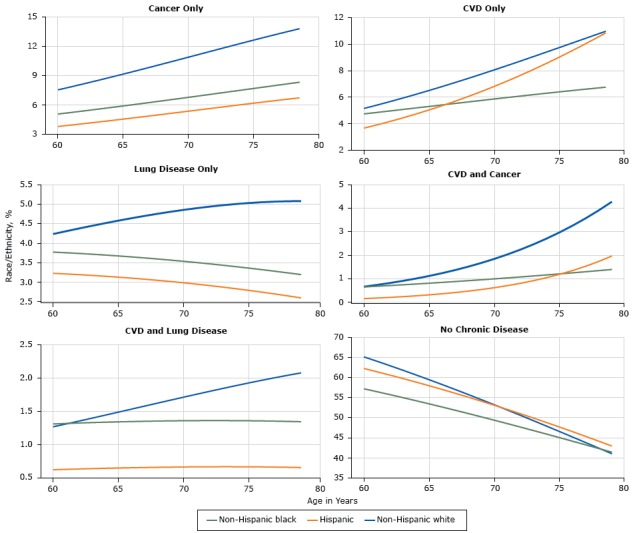
Hispanics and non-Hispanic blacks had the greatest prevalence of diabetes, and non-Hispanic whites had the greatest prevalence of cancer and chronic lung disease. The prevalence of multiple chronic diseases in an individual varied less by race/ethnicity. An exception was the prevalence of having both diabetes and CVD, which was higher among Hispanics and non-Hispanic blacks than non-Hispanic whites. Non-Hispanic blacks aged 65 years and 75 years had higher odds of having diabetes and cancer than non-Hispanic whites at the same ages. Hispanics had lower odds of having CVD with cancer or chronic lung disease than non-Hispanic whites. Women had a lower age-specific prevalence than men for most of the 11 single and multiple conditions. Most chronic diseases showed an inverse relationship with education and a higher prevalence in the South than in other regions.
Strong racial/ethnic differences exist in the prevalence of single chronic conditions, but differences are lower for prevalence of multiple conditions. Comparing races/ethnicities, the same disease dyads and triads may occur more often in different orders.
在美国,糖尿病、癌症、心血管疾病(冠心病、心脏病发作和心绞痛)和慢性肺部疾病(肺气肿、慢性支气管炎和慢性阻塞性肺疾病)是主要死亡原因。本研究的目的是评估这些疾病在 60 至 79 岁患有一种或多种这些疾病的人群中作为死亡原因的种族/民族差异。
我们使用了来自国家健康访谈调查的数据,该调查涉及 56290 名年龄在 60 至 79 岁的成年人,他们报告在 2006 年至 2014 年期间患有国家健康访谈调查评估的任何一种慢性疾病。我们比较了 11 种单一和多种疾病随年龄的趋势。分析采用多项逻辑回归模型。
西班牙裔和非西班牙裔黑人的糖尿病患病率最高,非西班牙裔白人的癌症和慢性肺部疾病患病率最高。个体中多种慢性疾病的患病率受种族/民族的影响较小。一个例外是同时患有糖尿病和心血管疾病的患病率,在西班牙裔和非西班牙裔黑人群体中高于非西班牙裔白人群体。与同年龄的非西班牙裔白人相比,65 岁和 75 岁的非西班牙裔黑人患有糖尿病和癌症的几率更高。与非西班牙裔白人相比,西班牙裔患有心血管疾病合并癌症或慢性肺部疾病的几率较低。在大多数 11 种单一和多种疾病中,女性的年龄特异性患病率低于男性。大多数慢性疾病与教育程度呈负相关,南部的患病率高于其他地区。
在单一慢性疾病的患病率方面存在明显的种族/民族差异,但在多种疾病的患病率方面差异较小。在比较种族/民族时,相同的疾病对可能以不同的顺序更频繁地出现。