Adebanjo Tolulope, Godfred-Cato Shana, Viens Laura, Fischer Marc, Staples J Erin, Kuhnert-Tallman Wendi, Walke Henry, Oduyebo Titilope, Polen Kara, Peacock Georgina, Meaney-Delman Dana, Honein Margaret A, Rasmussen Sonja A, Moore Cynthia A
MMWR Morb Mortal Wkly Rep. 2017 Oct 20;66(41):1089-1099. doi: 10.15585/mmwr.mm6641a1.
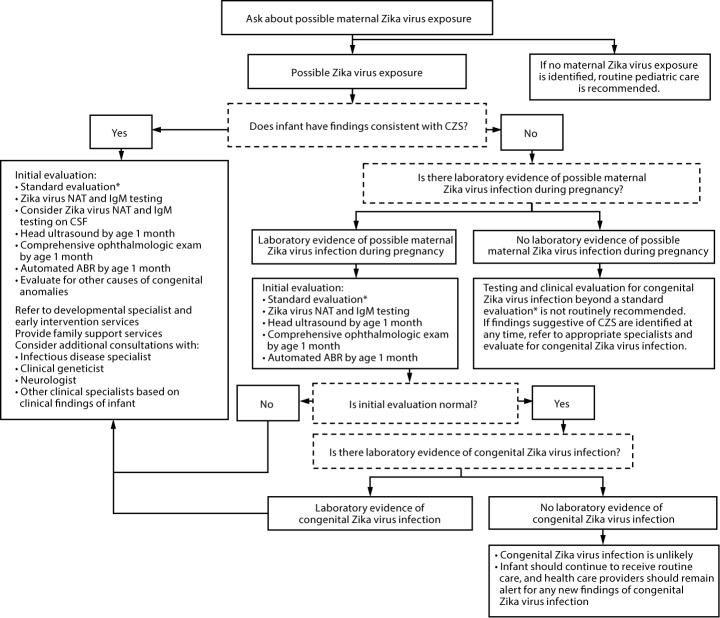
CDC has updated its interim guidance for U.S. health care providers caring for infants with possible congenital Zika virus infection (1) in response to recently published updated guidance for health care providers caring for pregnant women with possible Zika virus exposure (2), unknown sensitivity and specificity of currently available diagnostic tests for congenital Zika virus infection, and recognition of additional clinical findings associated with congenital Zika virus infection. All infants born to mothers with possible Zika virus exposure* during pregnancy should receive a standard evaluation at birth and at each subsequent well-child visit including a comprehensive physical examination, age-appropriate vision screening and developmental monitoring and screening using validated tools (3-5), and newborn hearing screen at birth, preferably using auditory brainstem response (ABR) methodology (6). Specific guidance for laboratory testing and clinical evaluation are provided for three clinical scenarios in the setting of possible maternal Zika virus exposure: 1) infants with clinical findings consistent with congenital Zika syndrome regardless of maternal testing results, 2) infants without clinical findings consistent with congenital Zika syndrome who were born to mothers with laboratory evidence of possible Zika virus infection, and 3) infants without clinical findings consistent with congenital Zika syndrome who were born to mothers without laboratory evidence of possible Zika virus infection. Infants in the first two scenarios should receive further testing and evaluation for Zika virus, whereas for the third group, further testing and clinical evaluation for Zika virus are not recommended. Health care providers should remain alert for abnormal findings (e.g., postnatal-onset microcephaly and eye abnormalities without microcephaly) in infants with possible congenital Zika virus exposure without apparent abnormalities at birth.
美国疾病控制与预防中心(CDC)已更新针对为可能感染先天性寨卡病毒的婴儿提供护理的美国医疗服务提供者的临时指南(1),以回应最近发布的针对为可能接触寨卡病毒的孕妇提供护理的医疗服务提供者的更新指南(2)、目前可用的先天性寨卡病毒感染诊断测试未知的敏感性和特异性,以及对与先天性寨卡病毒感染相关的其他临床发现的认识。所有在孕期母亲可能接触寨卡病毒*的婴儿,在出生时及随后每次健康儿童检查时都应接受标准评估,包括全面的体格检查、使用经过验证的工具进行适龄视力筛查以及发育监测和筛查(3 - 5),并在出生时进行新生儿听力筛查,最好采用听觉脑干反应(ABR)方法(6)。针对母亲可能接触寨卡病毒情况下的三种临床场景,提供了实验室检测和临床评估的具体指南:1)无论母亲检测结果如何,具有与先天性寨卡综合征相符的临床发现的婴儿;2)出生于有实验室证据表明可能感染寨卡病毒的母亲但无与先天性寨卡综合征相符的临床发现的婴儿;3)出生于无实验室证据表明可能感染寨卡病毒的母亲且无与先天性寨卡综合征相符的临床发现的婴儿。前两种场景中的婴儿应接受寨卡病毒的进一步检测和评估,而对于第三组婴儿,不建议进行寨卡病毒的进一步检测和临床评估。医疗服务提供者应警惕出生时无明显异常但可能接触先天性寨卡病毒的婴儿出现异常发现(例如,产后小头畸形和无小头畸形的眼部异常)。