Crowe Sally, Fenton Mark, Hall Matthew, Cowan Katherine, Chalmers Iain
Crowe Associates Ltd., 15 Chinnor Road, Thame, Oxon OX9 3LW UK.
UK DUETs, NHS Evidence, National Institute of Health and Social Care Excellence, Level 1A, City Tower, Piccadilly Plaza, Manchester, 4BD M1 UK.
Res Involv Engagem. 2015 Jun 25;1:2. doi: 10.1186/s40900-015-0003-x. eCollection 2015.
There is some evidence that there is a mismatch between what patients and health professionals want to see researched and the research that is actually done. The James Lind Alliance (JLA) research Priority Setting Partnerships (PSPs) were created to address this mismatch. Between 2007 and 2014, JLA partnerships of patients, carers and health professionals agreed on important treatment research questions (priorities) in a range of health conditions, such as Type 1 diabetes, eczema and stroke. We were interested in how much these JLA PSP priorities were similar to treatments undergoing evaluation and research over the same time span. We identified the treatments described in all the JLA PSP research priority lists and compared these to the treatments described in a group of research studies (randomly selected) registered publically. The priorities identified by JLA PSPs emphasised the importance of non-drug treatment research, compared to the research actually being done over the same time period, which mostly involved evaluations of drugs. These findings suggest that the research community should make greater efforts to address issues of importance to users of research, such as patients and healthcare professionals.
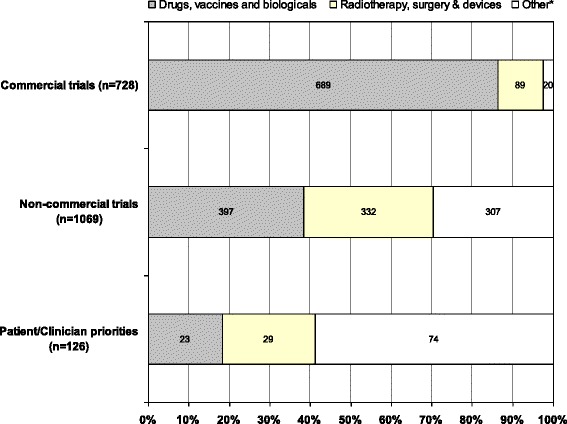
Comparisons of treatment research priorities identified by patients and clinicians with research actually being done by researchers are very rare. One of the best known of these comparisons (Tallon et al. Relation between agendas of the research community and the research consumer 355:2037-40, 2000) revealed important mismatches in priorities in the assessment of treatments for osteoarthritis of the knee: researchers preferenced drug trials, patients and clinicians prioritised non-drug treatments. These findings were an important stimulus in creating the James Lind Alliance (JLA). The JLA supports research Priority Setting Partnerships (PSPs) of patients, carers and clinicians, who are actively involved in all aspects of the process, to develop shared treatment research priorities. We have compared the types of treatments (interventions) prioritised for evaluation by JLA PSPs with those being studied in samples of clinical trials being done over the same period. We used treatment research priorities generated by JLA PSPs to assess whether, on average, treatments prioritised by patients and clinicians differ importantly from those being studied by researchers. We identified treatments mentioned in prioritised research questions generated by the first 14 JLA PSPs. We compared these treatments with those assessed in random samples of commercial and non-commercial clinical trials recruiting in the UK over the same period, which we identified using WHO's International Clinical Trials Registry Platform. We found marked differences between the proportions of different types of treatments proposed by patients, carers and clinicians and those currently being evaluated by researchers. In JLA PSPs, drugs accounted for only 18 % (23/126) of the treatments mentioned in priorities; in registered non-commercial trials, drugs accounted for 37 % (397/1069) of the treatments mentioned; and in registered commercial trials, drugs accounted for 86 % (689/798) of the treatments mentioned. Our findings confirm the mismatch first described by Tallon et al. 15 years ago. On average, drug trials are being preferenced by researchers, and non-drug treatments are preferred by patients, carers and clinicians. This general finding should be reflected in more specific assessments of the extent to which research is addressing priorities identified by the patient and clinician end users of research. It also suggests that the research culture is slow to change in regard to how important and relevant treatment research questions are identified and prioritised.
有证据表明,患者和医疗专业人员希望看到的研究内容与实际开展的研究之间存在不匹配。詹姆斯·林德联盟(JLA)的研究优先事项设定伙伴关系(PSP)旨在解决这种不匹配。在2007年至2014年期间,患者、护理人员和医疗专业人员组成的JLA伙伴关系就一系列健康状况(如1型糖尿病、湿疹和中风)中的重要治疗研究问题(优先事项)达成了共识。我们感兴趣的是,这些JLA PSP优先事项与同一时期正在评估和研究的治疗方法有多大程度的相似性。我们确定了所有JLA PSP研究优先事项清单中描述的治疗方法,并将其与一组公开注册的研究(随机选择)中描述的治疗方法进行比较。与同一时期实际开展的主要涉及药物评估的研究相比,JLA PSP确定的优先事项强调了非药物治疗研究的重要性。这些发现表明,研究界应做出更大努力,以解决对研究使用者(如患者和医疗保健专业人员)重要的问题。
将患者和临床医生确定的治疗研究优先事项与研究人员实际开展的研究进行比较的情况非常罕见。其中最著名的比较之一(Tallon等人,《研究界议程与研究消费者之间的关系》,355:2037 - 40,2000)揭示了在评估膝骨关节炎治疗方法的优先事项方面存在重要的不匹配:研究人员倾向于药物试验,患者和临床医生则优先考虑非药物治疗。这些发现是创建詹姆斯·林德联盟(JLA)的重要推动因素。JLA支持由患者、护理人员和临床医生组成的研究优先事项设定伙伴关系(PSP),他们积极参与该过程的各个方面,以制定共同的治疗研究优先事项。我们将JLA PSP确定为优先评估的治疗方法(干预措施)类型与同一时期正在进行的临床试验样本中研究的治疗方法进行了比较。我们使用JLA PSP生成的治疗研究优先事项来评估患者和临床医生确定为优先的治疗方法与研究人员正在研究的治疗方法平均而言是否存在重要差异。我们确定了前14个JLA PSP生成的优先研究问题中提到的治疗方法。我们将这些治疗方法与同期在英国招募的商业和非商业临床试验随机样本中评估的治疗方法进行比较,我们使用世界卫生组织的国际临床试验注册平台确定了这些样本。我们发现患者、护理人员和临床医生提出的不同类型治疗方法的比例与研究人员目前正在评估的比例之间存在显著差异。在JLA PSP中,药物仅占优先事项中提到的治疗方法的18%(23/126);在注册的非商业试验中,药物占提到的治疗方法的37%(397/1069);在注册的商业试验中,药物占提到的治疗方法的86%(689/798)。我们的发现证实了Tallon等人15年前首次描述的不匹配情况。平均而言,研究人员倾向于药物试验,而患者、护理人员和临床医生则更喜欢非药物治疗。这一总体发现应体现在对研究在多大程度上解决了患者和临床医生这些研究最终用户确定的优先事项的更具体评估中。这也表明,在确定和优先考虑重要且相关的治疗研究问题方面,研究文化的变化较为缓慢。